Background: Differences persist in cancer morbidity and mortality. Individuals of lower socioeconomic status (SES) suffer disproportionately from cancer compared with individuals with higher SES. Social determinants of health (SDOH) have become increasingly important for achieving optimal cancer outcomes. The Social Vulnerability Index (SVI) is a key measure relating to SDOH, which can help identify populations at increased risk for poor health. Cancer survivors report psychosocial distress and delaying or forgoing care because of cost. Financial distress is linked to patient outcomes, quality of life, compliance, and survival.
Objective: In July 2022, a National Cancer Institute–Designated Cancer Center (NCI-DCC) partnered with a third-party vendor to launch a patient financial assistance program. The program included screening all patients receiving systemic therapy administered at infusion centers to reduce financial hardship related to cancer treatment.
Method: The technology company deployed an artificial intelligence platform matching engine integrated with the electronic health record data to match patients with program opportunities. The patient assistance programs included copay assistance for patients treated in 18 distinct electronic medical record departments in hospital-based infusion centers. The technology company hired, trained, and deployed remote patient advocates who interacted with patients receiving treatments and evaluated each for potential qualification for financial assistance. The patient advocates were fluent in English and Spanish to assist with language barriers. Patient advocates identified eligible patients and, after obtaining consent, enrolled patients in philanthropic foundations and pharmaceutical company assistance programs. Patient advocates submitted claims, tracked the status of enrollment and re-enrollment, facilitated payments, and logged awards.
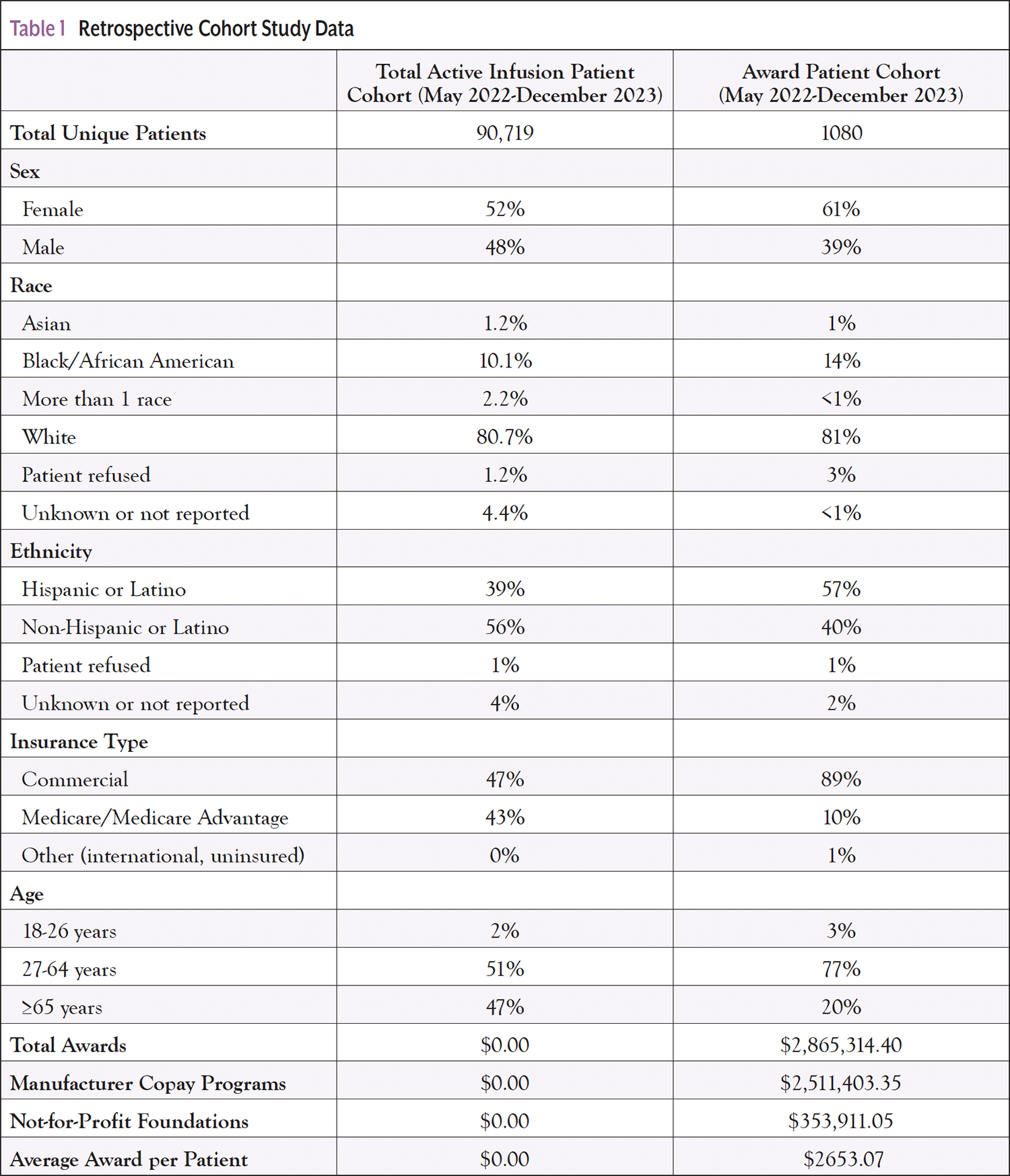
Results: A retrospective analysis of the period May 2022 to December 2023 was performed for the Award cohort (AC) that consisted of patients receiving philanthropic financial aid, including copay assistance and grants sponsored by drug manufacturers and not-for-profit foundations. For all patients receiving treatment in the NCI-DCC infusion centers, the total active infusion patient cohort was compared with the AC. Of the 90,719 unique patients who received systemic therapy in the NCI-DCC infusion centers, 1080 were matched for eligibility to patient assistance programs, resulting in $2,865,314.40 in total awards (AC). Of the total matched awards, 88% ($2,511,403.35) were from pharmaceutical company copay programs, and 12% ($353,911.05) were from not-for-profit foundations. The average matched award value was $2653.07 per patient. Patients who matched as eligible for assistance were predominantly commercially insured, 27 to 64 years old. These results represent the disproportionate availability of assistance for patients not covered by federally funded programs. Robust reporting facilitates efficient management and transparency.
Conclusion: A proactive patient financial assistance program can reduce financial distress, especially for those residing in high and medium-high SVI counties. Leveraging the expertise of a third party helps mitigate financial toxicity in the short term and can help drive more equitable cancer outcomes. The study is unique as it represents a diverse patient population that includes 10% Black/African American, 39% Hispanic/Latino, and a population at high risk for financial toxicity, given that 96% of AC patients reside in high or medium-high SVI counties.
Financial toxicity describes the excessive financial strain, burden, and distress patients and families experience when faced with a diagnosis like cancer. Significant disparities persist in cancer incidence, survival, morbidity, and mortality among populations in the United States. Individuals of lower socioeconomic status (SES) suffer disproportionately from cancer and other disease burdens compared with White individuals with higher SES.1 Financial toxicity was twice as frequent in patients aged 18 to 54 years compared with those patients older than 65 years.2
Patients experiencing financial toxicity are more likely to have psychosocial distress.1 Financial toxicity can lead to depression, anxiety, and additional stress during the cancer journey.3 Among 13,361 cancer survivor survey participants, 73% reported financial toxicity, including worries regarding the costs of paying for children’s college education, maintaining the standard of living, and medical expenses due to illness.4 Evidence-based interventions are needed to identify and mitigate financial toxicity among cancer patients to improve psychological well-being and overall outcomes.
Financial toxicity is linked with several clinically relevant patient outcomes, including treatment adherence and survival.5 Financial toxicity was associated with an increased risk of mortality among adults with cancer.5 In addition, Shankaran and colleagues demonstrated that for patients with cancer, there is an association between high out-of-pocket costs and an increased risk of experiencing adverse financial events, including late or missed credit card payments, which may have a long-standing, if not permanent, impact on their financial standing.6 Expanding access to patient assistance programs may mitigate financial toxicity due to the rapidly rising costs of cancer care.
Purpose
The Sylvester Comprehensive Cancer Center (SCCC), University of Miami Health System, a National Cancer Institute–designated cancer center (NCI-DCC), identified the need for better integration of financial advocacy into routine clinical practice. NCI-DCCs agree on better, more robust financial advocacy.7 The purpose of this study is threefold: (1) to identify the sociodemographic characteristics of patients benefiting from a proactive patient assistance program, (2) to compare them with the patients treated in SCCC infusion centers, and (3) to determine if the proactive patient assistance program successfully identified patients at the highest risk for financial toxicity. If the purposes are met, this supports an effective intervention to resolve patients’ unmet health-related costs, including injectable and infusion drug copayments.
SCCC has a sizable multidisciplinary cancer program serving a diverse patient population: 6565 analytic cases per year with 351 faculty physicians. To clearly define the characteristics of the patient population participating in patient assistance programs, the AC was compared with all patients treated in designated ambulatory infusion centers from May 2022 to December 2023 (the total active infusion patient cohort [TAIPC]). The AC demonstrated that 95% of the patients resided in high, 1% in medium-high, and 2% in low and medium-low Social Vulnerability Index (SVI) counties. Two percent of the AC represented non-Florida residents. Percent Federal Poverty Limit (%FPL) is used to identify patients’ socioeconomic status. Because %FPL was unavailable in the electronic health record (EHR), zip code/county data were used to determine the SVI score for the AC patient population. SCCC has a robust patient distress screening process. The My Wellness Check (MWC) program is designed to assess and triage real-time patient-reported outcomes of ambulatory oncology patients. Patients with a cancer diagnosis receive a questionnaire that addresses emotional, physical, nutritional, supportive, and practical needs 3 days before their office visit via their patient portal. Patients receive the initial questionnaire before their second visit to the SCCC and subsequent questionnaires not more frequently than every 30 days. The questionnaires are distributed in English or Spanish based on patients’ language preferences in the EHR. Data documented by Penedo and colleagues from October 2019 to January 2021 showed that 22% of the SCCC MWC questionnaires identified patients’ practical needs associated with financial toxicity.8
Given the substantial number of patients with unmet practical needs associated with financial toxicity, only 68.4% of the SCCC MWC alerts were completed by social workers in a 72-hour window.8 Staffing challenges, lack of knowledge regarding available resources, and the use of manual processes made it difficult to address all the patients’ needs within the desired time. Therefore, SCCC partnered with Atlas Health, a technology company that provides a full-service, artificial intelligence (AI)-powered patient advocacy solution. Atlas Health provides the patient advocates and technology platform to proactively match, enroll patients, and collect funds from medical philanthropic financial aid and pharmaceutical company assistance programs via a proprietary database, including thousands of programs representing more than $30 billion annually.9
Interventions
In July 2022, SCCC and Atlas Health partnered to launch a proactive patient financial assistance program. The program included screening all patients receiving systemic injectable and infusion therapy at SCCC infusion centers. The types of patient assistance programs included copay assistance from not-for-profit foundations and pharmaceutical company programs. The partnership did not include specialty pharmacy patient assistance and free drug programs.
Before the SCCC partnership with Atlas Health, there was a lack of coordinated patient assistance processes, and SCCC did not routinely utilize available resources. Patients were provided with their projected financial responsibility estimates only when requested. Many of the patients were unaware of the impending financial obligations, resulting in increased financial toxicity and patient dissatisfaction. Patients attempted to pursue financial assistance without professional guidance and often became frustrated with the process. In addition, SCCC did not have an established internal process to collect from external sources; therefore, patients were required to pay up front and obtain reimbursement independently.
Atlas Health deployed an AI-powered platform integrating with the SCCC EHR data, automatically matching patients with program opportunities using workflow automation, including prefilled application data and integrated email, text, and eFax. The technology company trained remote patient advocates fluent in English and Spanish who interacted with patients and evaluated each for potential qualification for financial assistance. SCCC offered translation services for other languages. Monthly meetings occurred between Atlas Health and SCCC to share reporting and facilitate efficient management and data transparency.
Evaluation
A retrospective analysis of the award period (May 2022-December 2023) compared AC and TAIPC patients. Of the 90,719 unique patients in the TAIPC, 1080 were matched for eligibility to patient assistance programs, resulting in $2,865,314.40 in the AC; 88% ($2,511,403.35) were from pharmaceutical company copay programs, and 12% ($353,911.05) were from not-for-profit foundations. The average matched award value was $2653.07 per patient. Awards included retroactive dates of service (prior to May 2022) based on program eligibility requirements.
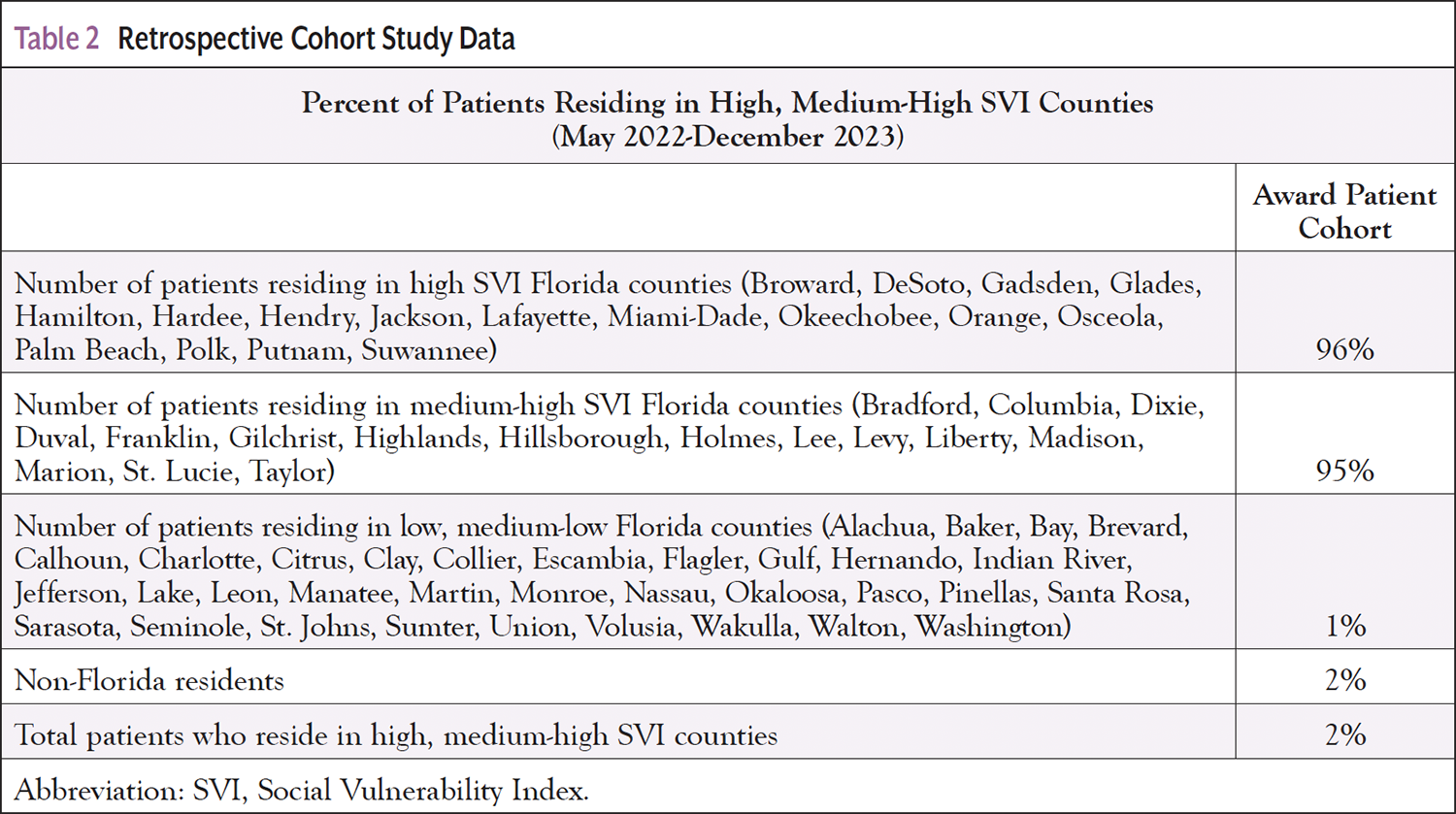
As displayed in Table 1, the TAIPC demographics comprised 52% females, 48% males, 10% Black or African American, 39% Hispanic or Latino, 47% commercial insurance, 43% Medicare/Medicare Advantage, 2% 18 to 26 years old, 51% 27 to 64 years old, and 47% ≥65 years old. Compared with the TAIPC, the AC demonstrated a higher percentage of female patients (61%), Black/African American patients (14%), and Hispanic/Latino patients (57%). The AC also represented a higher percentage of commercially insured patients (89%). The AC included a larger percentage of 27- to 64-year-old patients (77%), and a smaller percentage of patients ≥65 years old (20%). As shown in Table 2, 96% of the patients in the AC reside in counties with high or medium-high SVI.
Discussion
Recent studies have shown racial/ethnic and language disparities in access to patient assistance programs. Non-White and non-English–speaking patients were less likely to receive assistance than White and English-speaking patients.10 In contrast, our study demonstrated that the AC included a higher percentage of Black/African American and Hispanic/Latino patients compared with the TAIPC (Table 1). While further research is needed, these results suggest that culturally adapted processes help reduce access barriers for racial/ethnic minority populations.
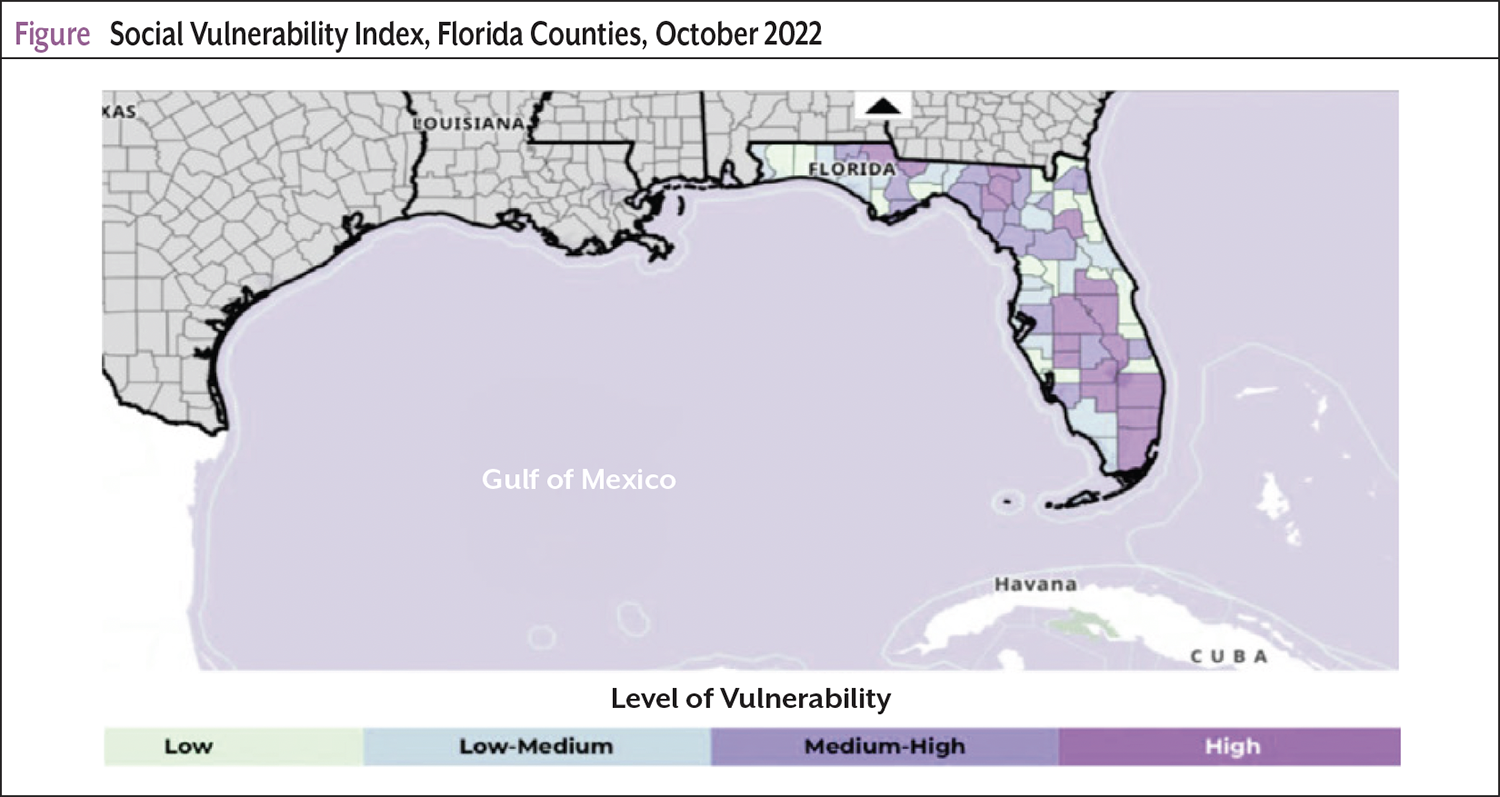
Social determinants of health (SDOH) have become increasingly important for achieving optimal cancer outcomes. The SVI is a key measure relating to SDOH, which can help identify populations at increased risk for poor health.11 The Agency for Toxic Substances and Disease Registry developed SVI using United States Census information to calculate SVI per county based on 4 key themes and 15 social factors, including socioeconomic status, household composition, disability, race/ethnicity, language, and housing or transportation status.11 A higher SVI score indicates greater social vulnerability linked to key barriers affecting overall wellness. The most socially vulnerable US counties have higher cancer mortality rates.12 Cancer patients in lower-income household groups are at high risk for financial toxicity.13 %FPL is used to identify patients’ socioeconomic status. Because %FPL was unavailable in the EHR, zip code/county data were used to determine the SVI score for the AC patient population (Table 2). The AC demonstrated that 96% of the patients resided in high, 1% in medium-high, and 2% in low and medium-low SVI counties; 2% of the AC represented non-Florida residents. Ninety-six percent of the patients who were matched as eligible for patient assistance programs represented the most vulnerable populations (Table 2; Figure).
Commercially insured patients aged 27 to 64 years are at high risk for financial toxicity and have increased access to patient assistance programs. The increased award distribution for those younger than age 65 represents the disproportionate availability of assistance for patients not covered by federally funded programs. Pharmaceutical company–sponsored copay programs provide direct financial assistance for eligible commercially insured patients and are unavailable for federal or state health insurance. Pharmaceutical company–sponsored copay programs help patients meet their financial responsibility incurred by injectable and infusion drug therapy.
While the eligibility requirements vary, most programs require the individual to demonstrate personal responsibility by submitting documentation of paid claims to generate awards. Many programs allow retroactive requests for infusions up to 180 days before enrollment—each program’s eligibility links to a specific drug. Patients on regimens that include multiple high-cost drugs must enroll in several programs, making applying for and collecting awards very time intensive. Patients with state or federally funded health insurance must rely on charitable foundations for assistance, limiting the availability of funds. As a result, Medicare-insured patients aged ≥65 years were underrepresented in the AC.
Accessing medical philanthropic aid through charitable foundations is more restrictive. Foundations can only help patients receiving treatment for indications for which there is an open disease fund. Disease funds for high-incidence cancers open and close very quickly. In 2018, 10% of Medicare beneficiaries, 5.6 million people, were covered by traditional Medicare with no supplemental coverage, including Medigap, employer-sponsored insurance, Medicaid, or Medicare Advantage.14 Also, the percentage of Medicare patients with no supplemental insurance at SCCC is 9% of the total Medicare population. These patients are at the most significant risk of incurring high medical expenses with a 20% patient responsibility.
Implementing a proactive patient assistance program may mitigate financial toxicity for patients and the risk of bad debt for institutions. High cost sharing and interruptions in employment related to a cancer diagnosis can create financial instability. The average matched grant per patient was $2653.07, which likely had a high impact. Grants greater than $2000 have been shown to decrease patients’ financial distress.15 Before the program launch, patients could not easily access financial assistance grants to offset their infusion bills, creating a greater risk of unpaid patient balances. Nationally, hospitals’ and health systems’ bad debt attributable to self-pay balances after insurance payments grew from 11% in 2018 to almost 58% in 2021.16 In addition, collection rates for patient balances exceeding $7500 fell to 17% in 2020, and uncompensated care increased by 47%.
Patient advocates completed program enrollment for 85% of matched patients and received grant funds via integration with the hospital’s billing system. Before the program launch, patients sought program websites to complete enrollment independently, resulting in poor access to resources. Atlas Health’s patient-facing bilingual patient advocates operated as extensions of SCCC. Program enrollment may require patient consent and specific documents for eligibility. The technology company made the process easier for patients by enabling them to provide consent and digitally upload photos of needed documents.
Limitations
The results of our study should be interpreted in the context of several limitations and lessons learned. First, the results represent a limited patient population, not including programs for free drugs or specialty pharmacies. Data from these programs are needed to understand the full impact of reducing patient financial liability due to patient assistance. There is an urgent need for patient advocacy to lobby for shared decision-making and financial transparency. There has been initial progress with the Hospital Price Transparency Rule and the No Surprises Act. However, a significant gap remains in patient education regarding financial responsibilities. Future studies should address the clinical outcomes of patients receiving patient assistance, such as the impact on unplanned care, psychosocial distress, and treatment adherence. In addition, further studies should address health system outcomes, such as the impact on care costs, bad debt, and the patient experience.
Conclusions
This study is one of the few studies to identify the composition of patients eligible for copay assistance to demonstrate the program’s impact. The study is unique as it represents a diverse patient population at high risk for financial toxicity. Our findings are significant because they highlight the benefit of a proactive review of infusion patients for assistance eligibility and the opportunity to reach more patients.
A proactive patient assistance program can increase access to financial resources for racial/ethnically diverse patients and those residing in high and medium-high SVI counties, resulting in reduced financial toxicity. Before launching the proactive patient assistance program for those not covered by the Hospital Price Transparency Rule and the No Surprises Act, SCCC staff discussed financial care estimates only after the patient requested it. Leveraging the expertise of a third party can reduce financial toxicity in the short term and facilitate equitable cancer outcomes.
References
- Dee EC, Nipp RD, Muralidhar V, et al. Financial worry and psychological distress among cancer survivors in the United States, 2013-2018. Support Care Cancer. 2021;29:5523-5535.
- Smith GL, Lopez-Olivo MA, Advani PG, et al. Financial burdens of cancer treatment: a systematic review of risk factors and outcomes. J Natl Compr Canc Netw. 2019;17:1184-1192.
- Yanez B, Perry LM, Peipert JD, et al. Exploring the relationship among financial hardship, anxiety, and depression in patients with cancer: a longitudinal study. JCO Oncol Pract. 2024;20:1776-1783.
- American Cancer Society. The Costs of Cancer Survivorship – 2022. Updated December 8, 2022. Accessed July 3, 2024. www.fightcancer.org/policy-resources/costs-cancer-survivorship-2022
- Yabroff KR, Han X, Song W, et al. Association of cancer history and medical financial hardship with mortality in the United States. J Clin Oncol. 2020;38(suppl). Abstract 86.
- Shankaran V, Li L, Fedorenko C, et al. Risk of adverse financial events in patients with cancer: evidence from a novel linkage between cancer registry and credit records. J Clin Oncol. 2022;40:884-891.
- Khera N, Sugalski J, Krause D, et al. Current practices for screening and management of financial distress at NCCN member institutions. J Natl Compr Canc Netw. 2020;18:825-831.
- Penedo FJ, Medina HN, Moreno PI, et al. Implementation and feasibility of an electronic health record-integrated patient-reported outcomes symptom and needs monitoring pilot in ambulatory oncology. JCO Oncol Pract. 2022;18:e1100-e1113.
- Atlas. Atlas Health Recognized in 2022 KLAS Emerging Solutions Top 20 Report. Accessed July 14, 2024. https://atlas.health/resources/2022-klas-emerging-solutions-top-20-report
- Ragavan MV, Swartz S, Clark M, et al. Access to financial assistance programs and their impact on overall spending on oral anticancer medications at an integrated specialty pharmacy. JCO Oncol Pract. 2024;20:291-299.
- Centers for Disease Control and Prevention and Agency for Toxic Substances and Disease Registry. Social Vulnerability Index. Updated August 27, 2024. Accessed December 30, 2024. www.atsdr.cdc.gov/community-stress-resource-center/php/resources/social-vulnerability-index.html
- Mehta A, Jeon WJJ, Hino C, et al. Association of U.S. county social vulnerability with cancer mortality. J Clin Oncol. 2022;40(suppl):6534.
- National Cancer Institute. Financial Toxicity and Cancer Treatment (PDQ)–Health Professional Version. Updated May 29, 2024. Accessed December 30, 2024. www.cancer.gov/about-cancer/managing-care/track-care-costs/financial-toxicity-hp-pdq
- Yabroff KR, Mariotto A, Tangka F, et al. Annual Report to the Nation on the Status of Cancer, Part 2: Patient Economic Burden Associated With Cancer Care. J Natl Cancer Inst. 2021;113:1670-1682.
- Ragavan MV, Mora RV, Winder K, et al. Impact of a comprehensive financial resource on financial toxicity in a national, multiethnic sample of adult, adolescent/young adult, and pediatric patients with cancer. JCO Oncol Pract. 2023;19:e286-e297.
- Hudson C. Insured patients become top reason for bad debt at providers. Modern Healthcare. Updated August 23, 2022. Accessed July 20, 2024. www.modernhealthcare.com/finance/insured-patients-become-top-reason-bad-debt-providers
Copyright © 2025 Journal of Oncology Navigation & Survivorship. Reprinted with permission.