NSCLC Overview
Non–small-cell lung cancer (NSCLC)—including squamous-cell carcinoma, adenocarcinoma, and large-cell carcinoma—accounts for 80% to 85% of all lung cancers.1 Of patients diagnosed with lung cancer (all types), 17% have localized disease (confined to the primary site), 22% have regional disease (spread to regional lymph nodes), 57% have metastatic disease, and 4% have an unknown stage.2
Effective screening for and diagnosis of NSCLC at an early stage increases the likelihood of successful treatment and improved outcomes.3,4 The National Comprehensive Cancer Network® (NCCN®) defines early-stage NSCLC as stage I and II with negative nodes, locally advanced as stages II and III with positive nodes, and metastatic disease as stage IV; the NCCN uses the International Association for the Study of Lung Cancer (IASLC) lung cancer staging system, which was adopted by the American Joint Committee on Cancer (AJCC).5 This article is focused on nonmetastatic (stage I-III) NSCLC.
Screening, Diagnosis, and Staging
For individuals with an increased risk for lung cancer (those aged 55-80 years with a ≥30 pack-year smoking history), annual screening via low-dose helical computed tomography (LDCT) is recommended by the US Preventive Services Task Force.6 Annual LDCT screening showed a 20% reduction in lung cancer–related mortality in this high-risk population, based on the National Lung Screening Trial (NLST), a large, randomized controlled study that included 53,454 individuals.6,7
An even greater survival benefit was shown in the NELSON Netherlands Trial, a population-based study of high-risk former and current smokers (13,195 men and 2594 women aged 50-74 years) that assessed screening compared with no screening at 1 year, 3 years, and 5.5 years.4 At the minimum follow-up of 10 years, screened men showed a 24% reduction in lung cancer mortality, and women, a 33% reduction.4 Screened individuals showed a low (1.2%) rate of false-positive tests. Moreover, 59% of all screening-detected lung cancers were diagnosed at stage IA or IB, compared with 13.5% of nonscreening-detected lung cancers.4
The accurate diagnosis and staging of NSCLC may involve several tests and procedures that guide patient-specific prognosis and treatment decisions. These tests and procedures, which commonly involve multiple members of the multidisciplinary healthcare team, include one or more of the following: history and physical examination; chest x-ray; laboratory and pathology tests (tissue, blood, urine); computed tomography/positron emission tomography (CT/PET) scan; sputum cytology; fine-needle aspiration biopsy; bronchoscopy with biopsy and transbronchial needle aspiration; thoracentesis; mediastinoscopy; video-assisted thoracic surgery and open surgical biopsy; and lymph node biopsy.5,8 Other tests, conducted on tissue samples, may include molecular testing for genetic features and immunohistochemistry to check for specific antigens (markers) and to identify the histological subtype of NSCLC (ie, adenocarcinoma, squamous-cell carcinoma, adenosquamous carcinoma, large-cell carcinoma, and sarcomatoid carcinoma).5,8 Reflexive biomarker testing (ie, EGFR, KRAS, ROS1, ALK fusion, RET fusion, MET, HER2, PD-L1, and others) is conducted for nonmetastatic NSCLC by some institutions, although it is not recommended in the NCCN Guidelines. These biomarker test results may be relevant for patients who are being enrolled in NSCLC clinical trials or maintained on record in the event of disease relapse.9
Treatment of Nonmetastatic NSCLC
Treatment considerations for NSCLC are based on several factors: the stage of disease; histological classification; the performance status, lung function, cardiovascular health, and individual needs (lifestyle and preferences) of the patient; and molecular features of the tumor (to select biomarker-targeted therapies for advanced/metastatic disease or for a clinical trial).10,11 Clinical trials may shed light on the evolving role of predictive and prognostic biomarkers at earlier stages of NSCLC.12
Accurate staging of NSCLC, based on a combination of clinical and pathological factors, is a cornerstone for treatment decisions.8 Findings from staging procedures—ie, anatomic features of the tumor, status and location of affected lymph nodes, surgical margin status, and pleural involvement—inform prognostic and treatment decisions.8
For patients who smoke, smoking cessation is essential to achieve the best treatment outcomes.11
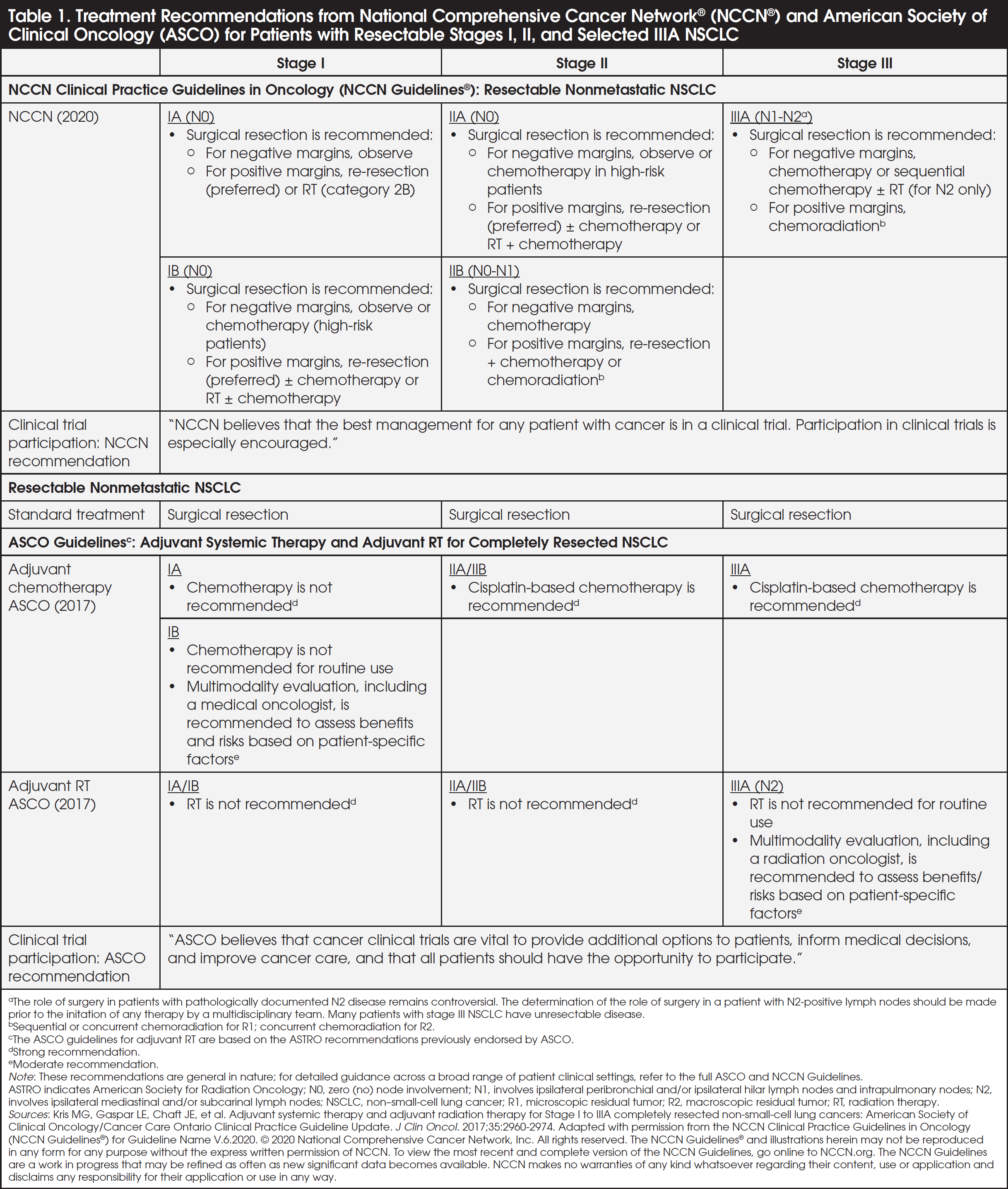
Treatment recommendations for patients with nonmetastatic NSCLC, based on clinical practice guidelines from the NCCN and the American Society of Clinical Oncology (ASCO), may include one or more of the following: surgery or systemic therapy (chemotherapy, radiation therapy [RT], and chemoradiation) (Table 1).5,10 A multidisciplinary treatment evaluation is recommended at key decision points along the NSCLC management pathway, particularly in candidates for multimodality treatment, toward the goal of selecting the most effective therapy and mitigating treatment-associated adverse effects.
Surgery for Resectable, Nonmetastatic NSCLC
Surgical resection is the standard-of-care treatment for resectable NSCLC.13 Surgical procedures for NSCLC include lobectomy, pneumonectomy, sublobular resection, bilobectomy, or sleeve resection.
Determining the resectability of NSCLC should involve an assessment by a thoracic surgeon, with input from the multidisciplinary team (MDT), and is based on 2 key factors: anatomic considerations (size and location of the tumor, extent of the disease, and the intricacies of removing the entire tumor) and the patient’s fitness for surgery (the patient’s age, cardiac and pulmonary health, comorbidities, and other factors that can lead to surgical complications).9,13 Subsequently, the patient is deemed resectable anatomically, unresectable anatomically, or medically fit or unfit for surgery.9
For patients with nonmetastatic NSCLC who undergo surgical resection, the 5-year overall survival rates by pathological stage are 83% and 71% for stages IA and IB, respectively, and 57% and 49% for stages IIA and IIB, respectively.14 However, for patients with stage IIIA NSCLC who underwent resection, the 5-year survival rate drops to 36%.
Among patients identified with nonmetastatic NSCLC, recurrence rates were more common at stage IIIA compared with stages I-II. Following curative-intent surgery, 52% (181/346) of patients with stage IIIA NSCLC experienced recurrence, compared with 20% (257/1294) of patients with stage I-II disease; moreover, distant recurrences were more common in patients with stage IIIA NSCLC than in patients with stages I-II NSCLC.15 The risk of recurrence for stage IIIA patients was highest within the first 2 years after resection (7 and 10 recurrences per 100 person-years in years 1 and 2, respectively), but remained substantial 4 years post-resection (2 per 100 person-years at year 4).15 In addition, the risk of second primary tumors increased each year (range 3%-6% per person-year) in the 2 to 5 years following curative resection in patients with nonmetastatic NSCLC.16
Surgery for NSCLC, like other surgical procedures, is associated with potential risks, including complications during and post-procedure, reactions to anesthesia, excessive bleeding, thrombotic events, pneumonia, and infections. Moreover, recovery from surgery may take weeks to months.17
There are broad variations in the quality of surgical approaches for lung cancer and the number of minimally invasive surgical techniques among US centers.18 Outcomes for surgery may be linked to the competency of the surgeon and surgical approach, as shown in the Society of Thoracic Surgeons (STS) General Thoracic Surgery Database (GTSD) study of 38,460 patients from 256 centers, which assessed the quality of care (risk-adjusted operative mortality and major morbidity) based on composite quality measures for all common lung cancer resections over a 3-year period (January 2015-December 2017).18 Surgeons who participated in the STS GTSD had an overall operative mortality rate of 1.3% and a major complication rate of 7.9%. In this study, 70.6% of the resections were minimally invasive approaches, and 22.3% were sublobar resections.18 Overall, the STS pulmonary resection composite shows that most centers that participate in the GTSD achieve acceptable perioperative outcomes. However, 3.7% of surgical programs perform below the average GTSD participant performance, whereas 6.5% perform above GTSD performance—factors that signal the need for consistent quality measures nationally.18
Treatment of Unresectable, Nonmetastatic NSCLC
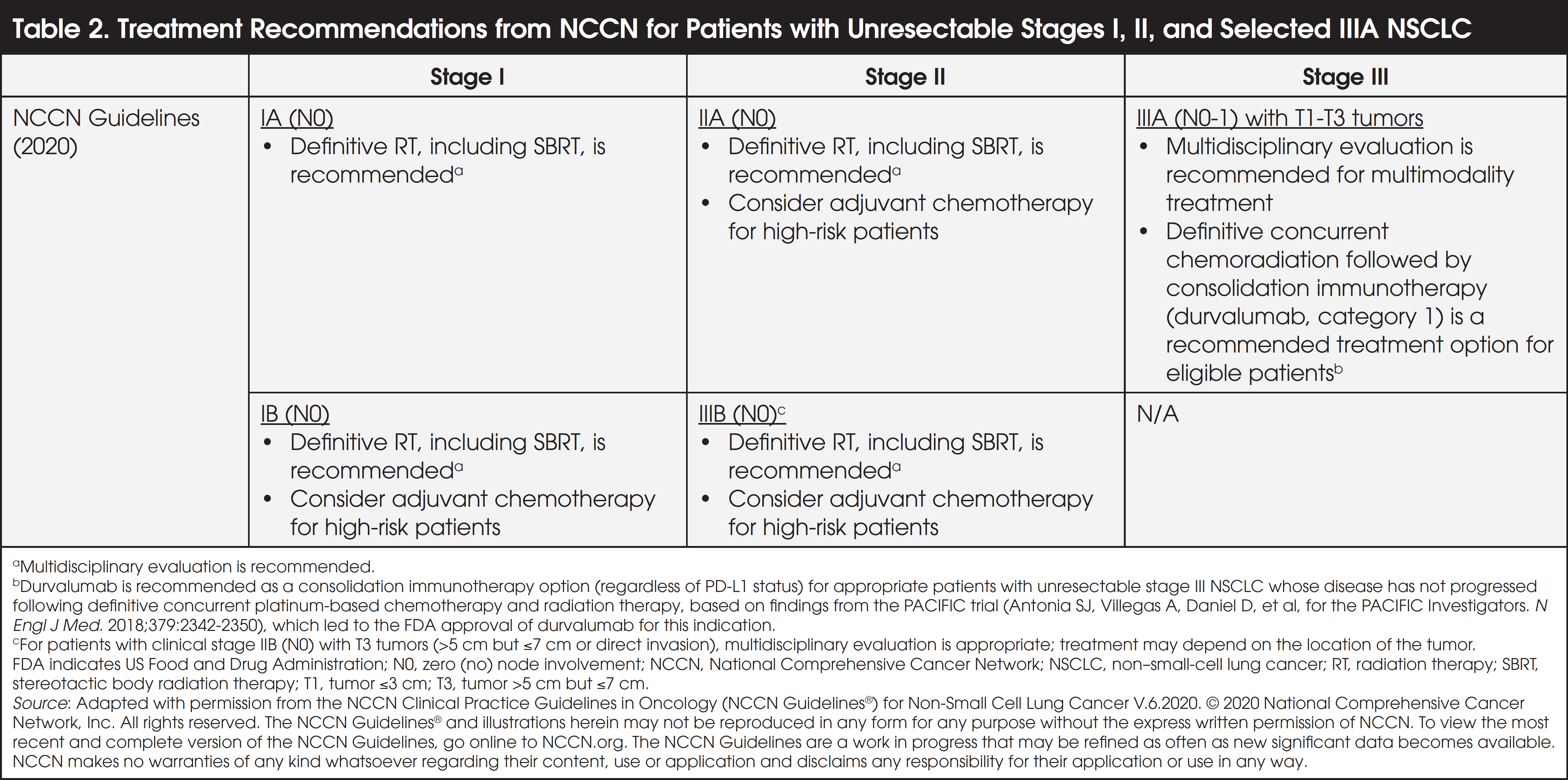
For patients with unresectable, nonmetastatic NSCLC, treatments recommended by NCCN include one or more of the following: chemotherapy (platinum-based), RT, including stereotactic body radiation therapy (SBRT), also known as stereotactic ablative radiotherapy (SABR), concurrent chemoradiation, and immunotherapy (for appropriate patients with stage III tumors) (Table 2).5 Some patients with unresectable stage disease (stage II and above) who are at high risk for recurrence may also receive adjuvant chemotherapy following RT. Definitive concurrent chemoradiation may be a treatment option for appropriate patients with unresectable stage III NSCLC.5 For patients with unresectable stage III NSCLC whose disease does not progress following definitive concurrent chemoradiation, consolidation immunotherapy with durvalumab, regardless of PD-L1 status, is a recommended treatment option, based on NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) and findings from the PACIFIC trial (Table 2).5
These guideline-based recommendations (Tables 1 and 2)5,10 are general in nature and do not capture the broad range of clinical settings and complexities involved in the management of nonmetastatic NSCLC (refer to the full NCCN Guidelines® and ASCO guidelines for detailed guidance). Participation in clinical trials is also strongly recommended by NCCN and ASCO as a treatment option for patients with NSCLC.5,10
Chemotherapy (Neoadjuvant and Adjuvant)
Treatment with chemotherapy alone either before or after surgical resection can improve outcomes in nonmetastatic disease; however, long-term survival rates remain suboptimal. In the NSCLC Meta-Analysis Collaborative Group analysis of patients with stage IB-IIIA NSCLC, the absolute overall survival improvement at 5 years was 5.0% for neoadjuvant chemotherapy based on a meta-analysis (N = 2385), and 5.4% for adjuvant chemotherapy, compared with no chemotherapy, based on a pooled data analysis (N = 4584).19,20 Moreover, neoadjuvant chemotherapy was associated with a 6% absolute improvement in recurrence-free survival at 5 years and a 10% absolute improvement in time to distant recurrence at 5 years.19 As suggested by this analysis, neoadjuvant chemotherapy may reduce the tumor size, increase the operability of the tumor, and eliminate micrometastases. Conversely, neoadjuvant chemotherapy may lead to delays that impact the ability to perform a complete resection.19
In the NATCH study (Felip and colleagues), no statistically significant difference in 5-year disease-free survival rate was shown between neoadjuvant chemotherapy plus surgery compared with adjuvant chemotherapy plus surgery (38.3% vs 36.6%, respectively) in patients with stages IA to IIIA (T3N1) NSCLC (N = 624). However, treatment compliance was significantly greater in the neoadjuvant arm; 90% of patients in the neoadjuvant arm received the 3 planned chemotherapy cycles, whereas 60% in the adjuvant arm received the 3 planned chemotherapy cycles.21
Platinum-based doublet chemotherapy for NSCLC is associated with potential adverse effects, including hair loss, weight change, loss of appetite, nausea and vomiting, diarrhea or constipation, fatigue, and an increased risk for infection and bleeding; moreover, some chemotherapies (ie, cisplatin, docetaxel, paclitaxel) are associated with an increased risk for peripheral neuropathy.22
Radiation Therapy/SBRT and Chemoradiation
Among patients with nonmetastatic NSCLC who are not candidates for surgery, treatment with SBRT achieved a >90% rate of local tumor control at 2 to 3 years.23,24 In the RTOG 0236 study in patients with unresectable, stage I-IIA NSCLC (N = 55), the 3-year overall survival and disease-free survival rates with SBRT were 55.8% and 48.3%, respectively; and the 5-year overall survival and disease-free survival rates were 40.0% and 25.5%, respectively.24,25
In another study (Palma and colleagues), patients with stage I NSCLC (N = 40) who underwent neoadjuvant SBRT followed by surgery 10 weeks later showed a lower-than-expected pathologic complete response rate of 60%.26 The study authors concluded that additional treatment approaches are needed to reduce the risk of regional and distant metastases and that further studies are warranted on SBRT followed by surgery and SBRT and immunotherapy in patients with early-stage (nonmetastatic) NSCLC.26
In a meta-analysis of patients with unresected, locally advanced (stages IIIA, IIIB) NSCLC (N = 1205), concomitant chemoradiation was associated with an absolute survival benefit compared with sequential chemoradiation of 5.7% at 3 years (23.8% vs 18.1%, respectively) and 4.5% at 5 years (15.1% vs 10.6%, respectively).27
Although SBRT for NSCLC is generally well-tolerated, SBRT-associated toxicities can affect the central airway, chest wall, aorta, and esophagus and can lead to pneumonitis or radiation-induced neuropathies.28 Other possible side effects of SBRT include fatigue, nausea and vomiting, weight loss and poor appetite, and skin changes in the area being treated.29
Immunotherapy
In the PACIFIC trial (Antonia and colleagues), immunotherapy with durvalumab, a PD-L1 inhibitor, demonstrated a significantly longer overall survival at 2 years compared with placebo (66.3% vs 55.6%, respectively; hazard ratio = 0.68) when administered as consolidation treatment after concurrent chemoradiotherapy in patients with stage III, unresectable NSCLC (N = 709). The median duration of progression-free survival was 17.2 months in the durvalumab group versus 5.6 months in the placebo group.30 These study results led to the US Food and Drug Administration (FDA) approval of durvalumab to treat patients with unresectable stage III NSCLC whose disease has not progressed following concurrent platinum-based chemotherapy and RT.31
The most common adverse reactions associated with immunotherapy for NSCLC include cough, fatigue, pneumonitis/radiation pneumonitis, upper respiratory tract infections, dyspnea, and rash.31 In the overall treatment of cancer, immunotherapy (immune checkpoint inhibitors) can affect the skin, gastrointestinal tract, and multiple other systems, including cardiovascular, pulmonary, endocrine, renal, hepatic, neurological, or ocular systems.32 Appropriate management approaches are detailed in the ASCO guidelines for managing adverse events associated with immune-oncology therapies.32
Unmet Needs in Nonmetastatic Stage NSCLC
Over the past 14 years, mortality from lung cancer has declined substantially with 16,547 fewer deaths annually in 2019 than in 2005.2,33 Despite improvements in overall survival and advances in the screening, staging, and treatment of NSCLC, the overall 5-year relative survival rate for patients with all stages of NSCLC is 24%.34 The relative 5-year survival rate by stage is as follows: stage I, 54%; stage II, 35%; stage IIIA (ipsilateral node involvement), 10%-15%; stage IIIB (contralateral lymph-node involvement), <5%; and stage IV, <2%.35
Delays in establishing a definitive diagnosis of NSCLC from the time of the initial diagnostic test may impact outcomes for patients whose disease is untreated and may progress during the delay period.36 A registry-based study showed that more than 90% of patients experienced a 5- to 6-month delay in a definitive NSCLC diagnosis following their first diagnostic test, signaling the need to improve the time to diagnosis.36
NSCLC represents a heterogeneous group of diseases—at the genetic, epigenetic, and cellular levels—that warrant more effective therapies and additional clinical trials.37 Chen and colleagues propose a need for “integrated therapy”—a genotype-directed, carefully selected combination that improves the immune response, inhibits tumor growth, and blocks key cellular interactions implicated in NSCLC.37 Despite advancements in treatment and improvements in survival, there remains a marked need for earlier diagnosis, novel therapies/combination options, and clinical studies—toward the goal of preventing or delaying disease progression in patients with nonmetastatic NSCLC. Moreover, best practices for a multidisciplinary approach to the management of NSCLC can provide a framework for identifying and addressing the patient’s evolving needs on a timely basis and for selecting the appropriate treatment—particularly therapies with fewer adverse effects that are better tolerated by the patient—at the appropriate time points.
Merits of a Multidisciplinary Approach to Nonmetastatic NSCLC
Optimal cancer care demands the collaboration of a MDT at key intervals along the journey of the patient with nonmetastatic NSCLC (Figure).9,38,39 The composition of the MDT may change, depending on the patient’s needs along the decision pathway; members of the MDT may include medical oncologists, surgical oncologists, radiation oncologists, thoracic surgeons, pulmonologists, thoracic radiologists, pathologists, oncology nurses, nurse navigators, social workers, and other experts.
Multidisciplinary evaluation and decision-making are at the core of individualized patient care in nonmetastatic NSCLC. MDT collaboration is essential to address barriers earlier, facilitate integration of clinical practice guidelines/pathways, establish accurate diagnosis/stage, determine tumor resectability, and provide guidance on the sequencing and timing of local and systemic therapies, particularly when multiple modalities are involved. Routinely held MDT tumor boards provide an effective forum to discuss the patient’s case, represent the patient’s evolving needs, and reach consensus as to next steps.
Although an MDT approach is vital across the entire continuum of care in NSCLC, it is particularly important in the management of nonmetastatic NSCLC. Collaboration of the MDT—across multiple specialties, including oncology, radiology, pulmonology, surgery, pathology, and nursing—plays a crucial role in complex decision-making about diagnostic imaging, pretreatment evaluation, resectability (assessment of comorbidities and surgical risk), selecting the appropriate treatment or combination treatment at the appropriate time, and minimizing treatment toxicities, particularly in the setting of multimodality therapies (see Figure 1 and the Best Practices in the MDT Management of Nonmetastatic NSCLC section).9,39 Vigilant patient follow-up by members of the MDT after curative-intent surgery may play a crucial role in improving outcomes for patients with nonmetastatic NSCLC, based on its role in the timely detection and prompt treatment of new primary tumors and disease recurrence (see Table 3 and the Best Practices in the MDT Management of Nonmetastatic NSCLC section).5,40
An MDT approach may be particularly consequential in stage III disease, given the degree of nodal involvement, varying prognoses, and multifaceted treatment decisions involved at this stage.41 For patients with stage III disease who require surgery, radiotherapy, and systemic therapy, MDT collaboration can help optimize patient-tailored treatment plans, including the appropriate sequence and timing of treatments/combinations.41 A registry-based study of patients with stage III NSCLC (N = 109) who were treated at an institution’s multidisciplinary thoracic clinic showed improved pathological mediastinal staging, fewer cases of unsuspected stage NII disease at the time of surgery, reduced delay in initial treatment, and greater adherence to the institution’s clinical pathways.42 Although multiple factors play a role in outcomes, the median overall survival for patients in the multidisciplinary clinic was 17 months compared with 14 months for patients managed outside of the multidisciplinary clinic (P = .054).42
Overall, an MDT approach to managing patients with lung cancer was associated with improved outcomes, as demonstrated in a recent study (Bilfinger and colleagues).43 The study spanned 14 years (2002- 2016) and evaluated survival benefit in 1956 patients in the MDT program and 2315 patients receiving traditional care. The MDT included a medical oncologist, a radiation oncologist, a thoracic surgeon, 2 dedicated nurse practitioners, and others. Notably, 50.5% in the MDT cohort and 19.7% in the traditional care cohort had stage I-II disease, respectively, whereas 25.8% and 20.0% had stage III disease, respectively.43 Overall, patients in the MDT program showed a significant 5-year survival advantage, compared with those receiving traditional care (33.6% vs 23.0%, respectively; P <.001).43 Although this study was nonrandomized, it included stage-stratified and propensity-matched assessments to mitigate potential biases in disease severity between the MDT and the traditional care group. In both analyses, the MDT program showed a survival benefit, regardless of stage.43
In another study, weekly MDT tumor boards were correlated with clinical trial participation of patients with lung cancer, but not with overall survival benefit.44 In addition, patients with stage I-II NSCLC who were discussed at weekly tumor boards were more likely to receive curative-intent surgery (guideline-recommended) compared with those whose cases were discussed less frequently or not at all at tumor boards.44
Best Practices in the MDT Management of Nonmetastatic NSCLC
Characteristics of an Effective MDT
According to Soukup and colleagues, an effective MDT has specific characteristics, including45:
- Participation of key MDT members; routine MDT meetings/tumor boards at a designated meeting room
- Team-based culture of mutual trust and respect; organizational support (funding; resources)
- Leadership by a chair or assigned organizer (ie, coordinated and facilitated by an oncology nurse navigator [ONN])
- Appropriate premeeting preparation and selection of cases for discussion
- Adequate representation of patient-centered views and preferences
- Clinical decision-making pathway; evidence-based guidelines and treatment protocols
- Data collection and analysis to foster learning and improve patient outcomes
- Post-meeting follow-up to coordinate the patient’s needs/services; ongoing clear communication among the MDT members and with the patient
The ONN is a vital member of the MDT who can lead the MDT, integrate best practices, and streamline processes toward improving patient outcomes.
Oncology Nurse Navigators’ Role in Patient-Centered Care
ONNs play a central, proactive role in advocating for patients, “navigating” them through the multilayered cancer care journey—from screening to diagnosis to treatment to symptom and side-effect monitoring, through the post-treatment follow-up, and beyond (Figure 1).9,39 As the primary liaison for the MDT and relevant departments, the ONN monitors processes for needless gaps and delays, works with the MDT to formalize clinical pathways (based on clinical practice guidelines), participates in patient outcome data collection and analysis, and addresses barriers to timely care.46,47
As the main point of contact for patients with cancer, the ONN’s multiple responsibilities include building trusted relationships with patients, educating patients and communicating with them regularly, attending relevant patient appointments and participating in tumor board/other meetings, identifying the patient’s psychosocial concerns, and providing needed resources.46 ONNs also play a role in increasing the patient’s awareness and understanding of clinical trials and facilitating access to clinical trials.48
Nurse navigator support for patients with recently diagnosed cancers, including lung cancer, has shown significant improvement in the patient’s overall care experience and a significant reduction in problems surrounding care coordination, health information, and psychosocial support.49 Implementation of an ONN-driven interdisciplinary tumor board and a guidelines-based clinical pathway was associated with a 37% increase in the diagnosis of early-stage nonmetastatic NSCLC at one facility over an 18-month period.50 This program succeeded in improving adherence to clinical practice guidelines and standardizing care for patients with NSCLC.50
MDT Role at Key Intervals in the Management of Nonmetastatic NSCLC
In nonmetastatic NSCLC, MDT collaboration is particularly important at clinical assessment, diagnosis, pretreatment evaluation, determination of operability, and patient follow-up (surveillance) after curative-intent treatment. The NCCN Guidelines recommend a multidisciplinary approach at specific phases and disease stages along the patient’s continuum of care, as follows5:
- Diagnosis of Stage I-III NSCLC. A multidisciplinary diagnostic team should thoroughly evaluate all findings and patient-specific factors to establish an accurate NSCLC diagnosis before any treatment is initiated. For optimal diagnosis and follow-up strategy of patients with suspected NSCLC, the MDT evaluation should include a thoracic surgeon, thoracic radiologist, and pulmonologist.
- Determination of Resectability, Surgical Staging, and Pulmonary Resection. A thoracic surgeon should participate in MDT discussions and tumor boards. When possible, the patient should have tissue confirmation of NSCLC before nonsurgical treatment. An interventional radiologist, thoracic surgeon, and pulmonologist should participate in pretreatment evaluation to determine the safest and most effective approach and to achieve a consensus as to whether a biopsy is too risky and whether the patient with early-stage unresectable disease can proceed with definitive RT, including SABR, without tissue confirmation of NSCLC.
- Stage II or greater NSCLC. The patient should be referred to a medical oncologist for evaluation; the medical oncologist participates in the MDT. For patients considered to have stage IIB and stage III tumors, where more than one treatment modality (surgery, RT, or chemotherapy) is considered, a multidisciplinary evaluation should be performed.
- Stage IIB and Stage III Tumors in Patients Who Are Candidates for Multimodality Therapies (Surgery, RT, or Chemotherapy). An MDT evaluation is warranted to discuss treatment.
- Stage III NSCLC. Resectability should be determined in multimodality settings before treatment is initiated; a previous MDT consultation is particularly important when surgery is being considered for patients with stage III disease.
- Stage IIIA (Unresectable). Consider referring the patient to a radiation oncologist; treatment delays should be averted.
- Unresectable Tumors, Patients Who Refuse Surgery, or Those with High Surgical Risk. Some of these patients with early-stage disease are candidates for RT, including SABR. The radiation oncologist should provide input as part of the MDT.
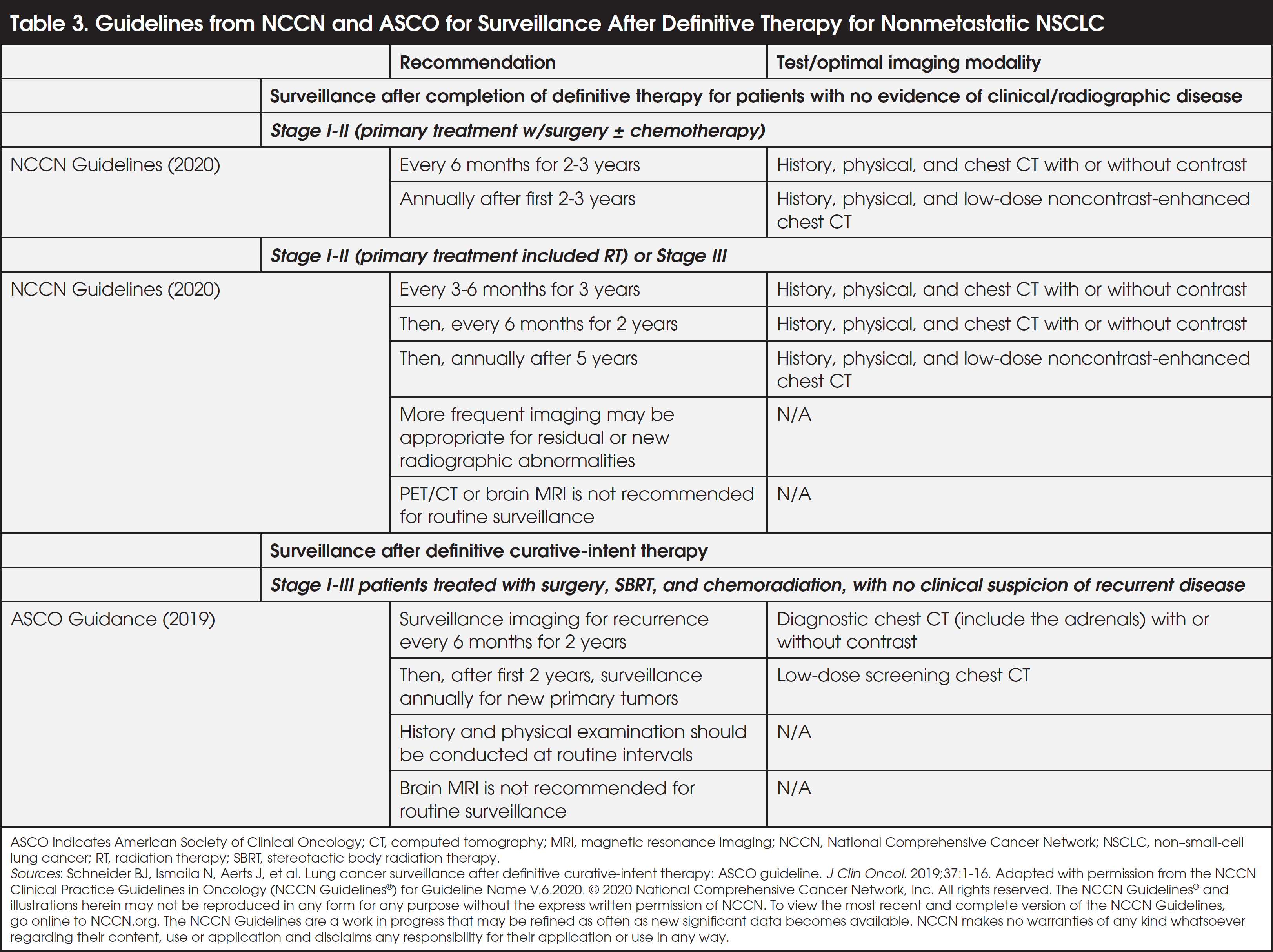
For patients with stage I-IIIA NSCLC, the risk for disease recurrence is greatest in the first 2 years after curative-intent treatment.15 Surveillance for early detection of recurrences and new tumors using radiographic imaging is a crucial patient follow-up step toward improving outcomes. For patients with no evidence of disease after primary treatment, the NCCN Guidelines recommend surveillance for disease recurrence every 6 months for the first 2 to 3 years for patients with stage I-II NSCLC and every 3 to 6 months for 3 years for patients with stage III NSCLC and those with stage I-II NSCLC whose primary treatment included RT (Table 3).5,40 These patient follow-up guidelines can be integrated into standardized clinical pathways, with subsequent clinical decisions evaluated in an MDT setting.
The Patient’s Journey in Nonmetastatic NSCLC
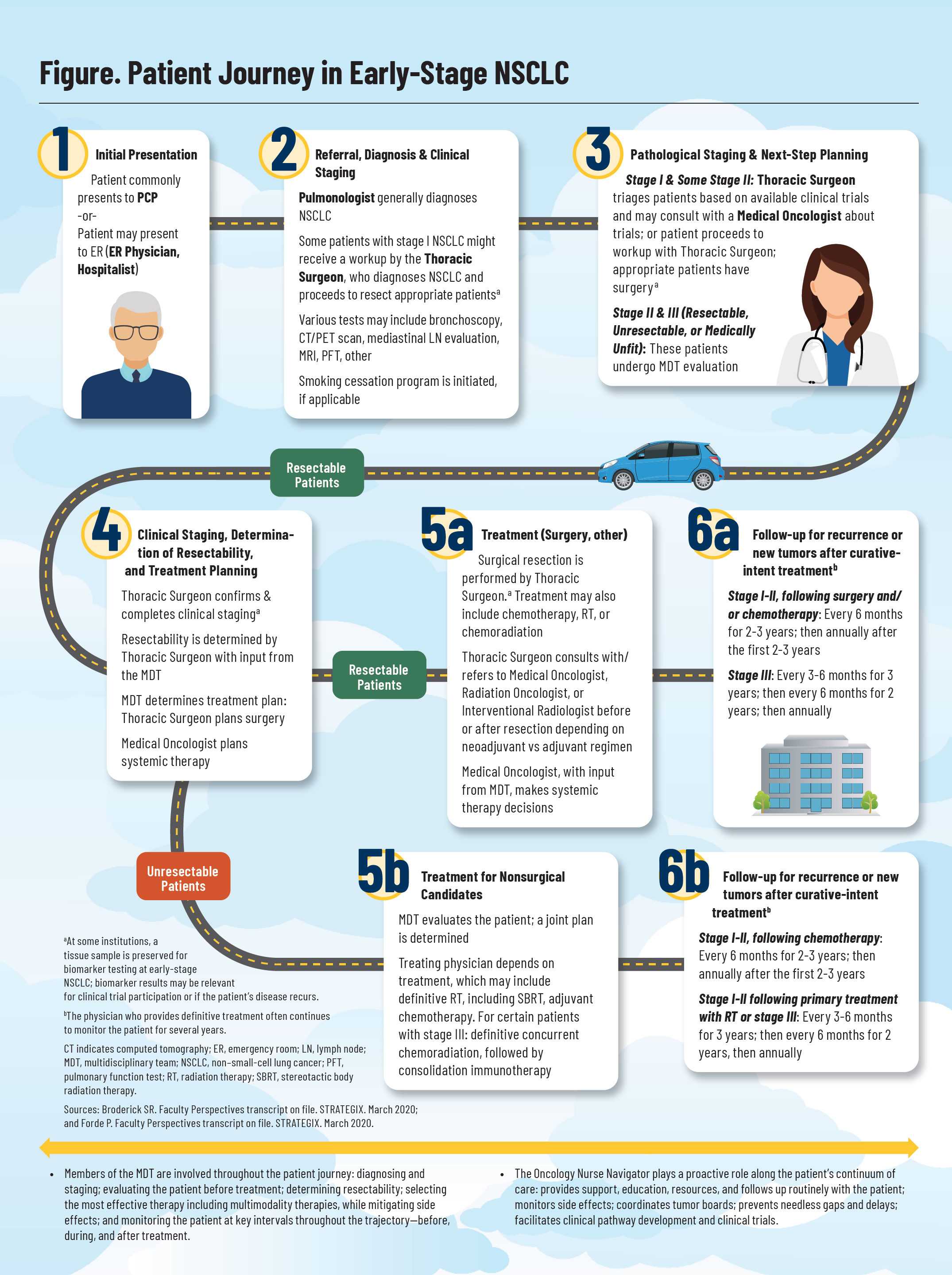
The patient’s pathway during nonmetastatic NSCLC is represented in Figure 1.9,39 The patient initially presents with symptoms to the primary care physician or to the emergency department. The patient is then commonly referred to the pulmonologist, who diagnoses NSCLC; some patients with stage I disease may be seen by a thoracic surgeon for a workup and determination of pathologic staging. Generally, the thoracic surgeon or the MDT determines whether the patient is resectable, unresectable, and medically fit for surgery. At the time of diagnosis and staging, some institutions preserve a tissue sample and conduct biomarker testing for patients with nonmetastatic NSCLC. These biomarker results can be useful if the patient is subsequently enrolled in a clinical trial or the patient has a disease recurrence.
The treatment path for patients with resectable nonmetastatic NSCLC differs from those with unresectable disease (Figure 1, Table 1, Table 2).5,9,10,39 Resectable and borderline-resectable patients are clinically staged and seen by the thoracic surgeon and in some cases, the medical oncologist, particularly if systemic therapy is indicated. Most patients with stage II and III NSCLC are evaluated by the MDT, including a radiation oncologist or interventional radiologist if RT is appropriate.
Patients with unresectable disease or those who are deemed medically unfit for surgery are evaluated by the MDT, and a joint treatment plan is formulated. The lead physicians on the MDT depend on the treatment plan selected. In some cases, if the tumor is conducive to SBRT and the mediastinum is node-negative, the radiation oncologist will perform SBRT. If the tumor is not suitable for SBRT, the patient may be seen by both a radiation oncologist for RT and by the medical oncologist for systemic chemotherapy.
Patient follow-up (surveillance) is a key aspect of the treatment journey (see also Table 3).5,40
Future Landscape in the Treatment of Nonmetastatic NSCLC
For patients with nonmetastatic NSCLC, effective new treatment options with favorable safety profiles may improve the suboptimal long-term outcomes achieved with current standard-of-care therapies. According to Foster and colleagues, further clinical trials are warranted to assess optimal treatment approaches for immunotherapy and multimodality treatments, including RT.51
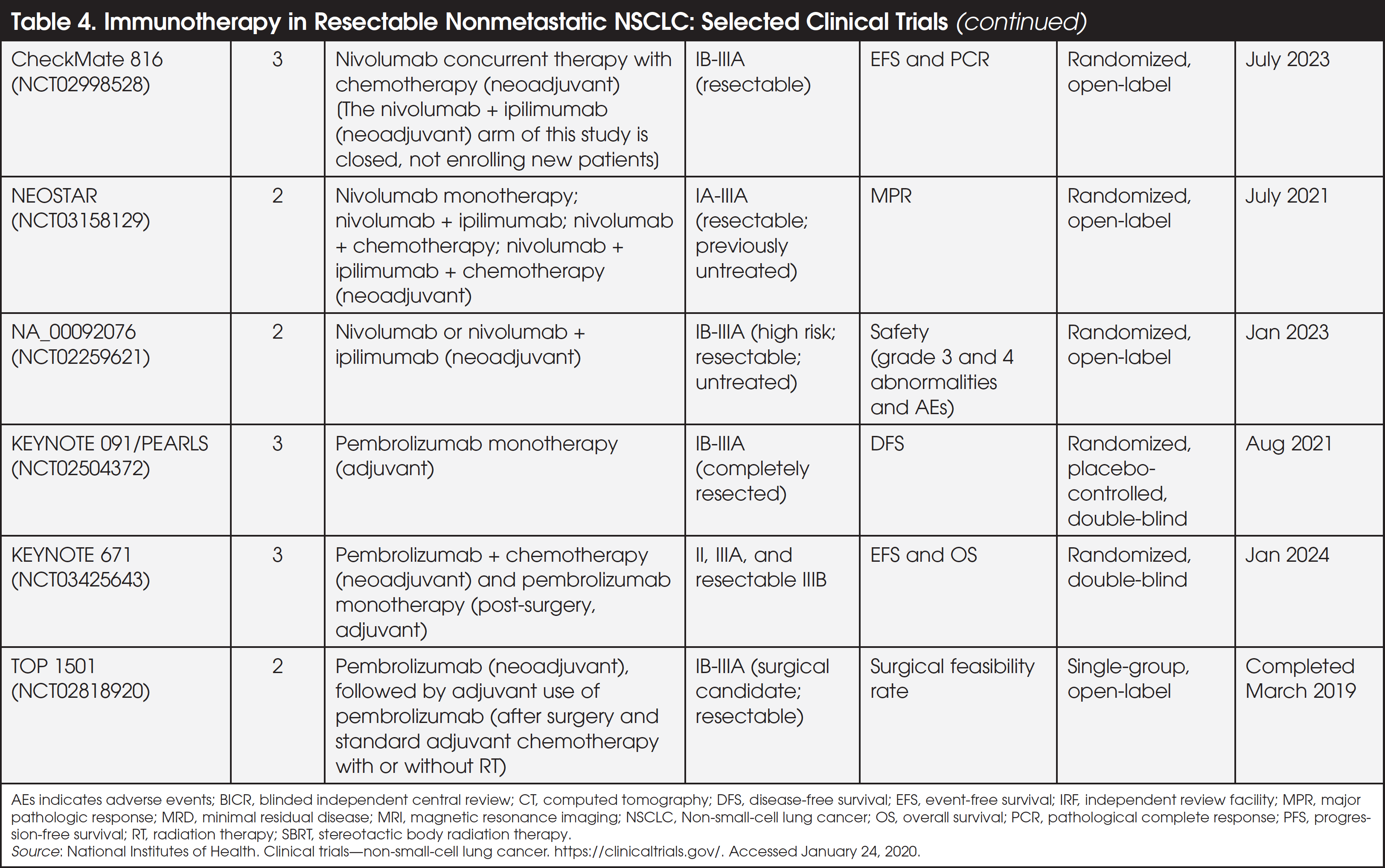
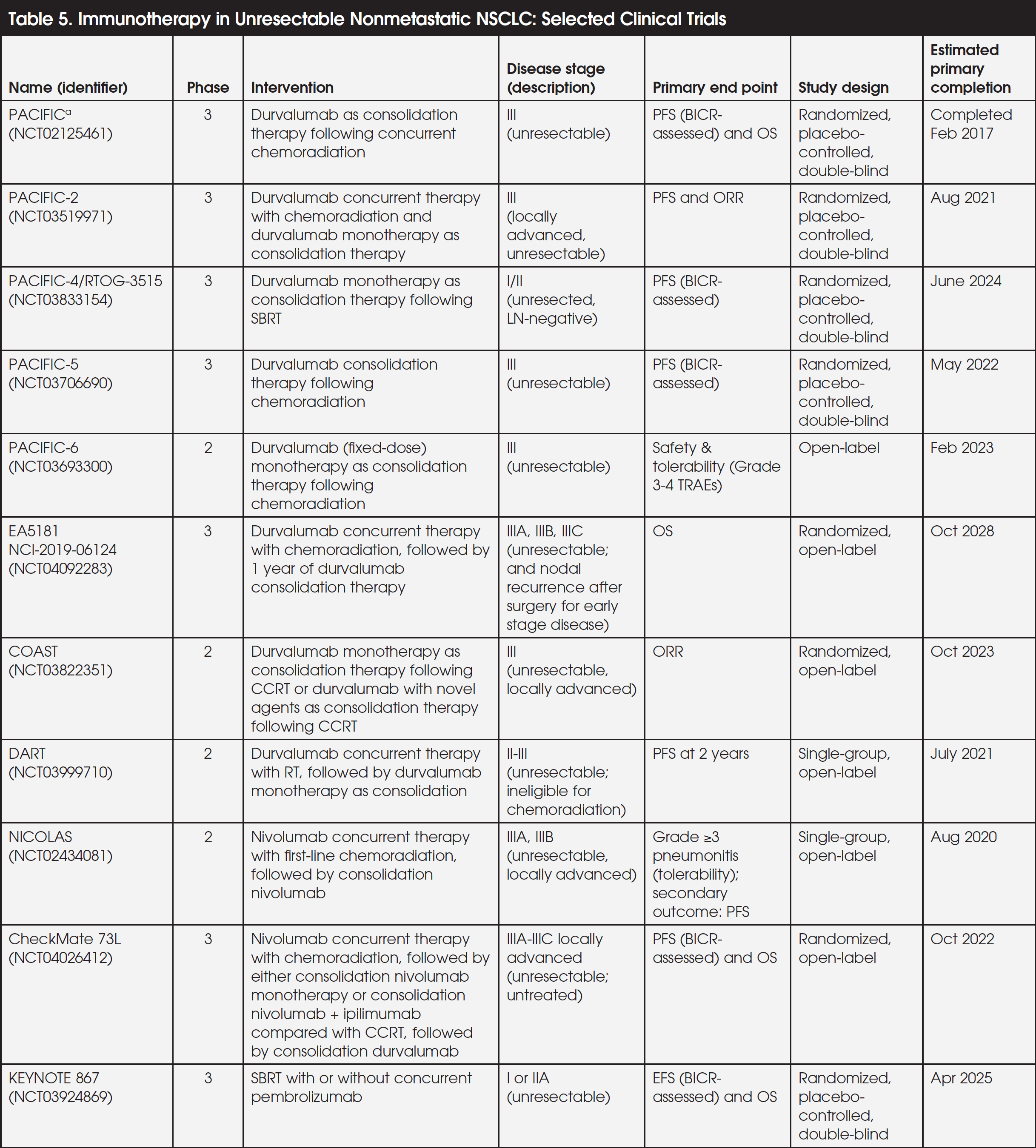
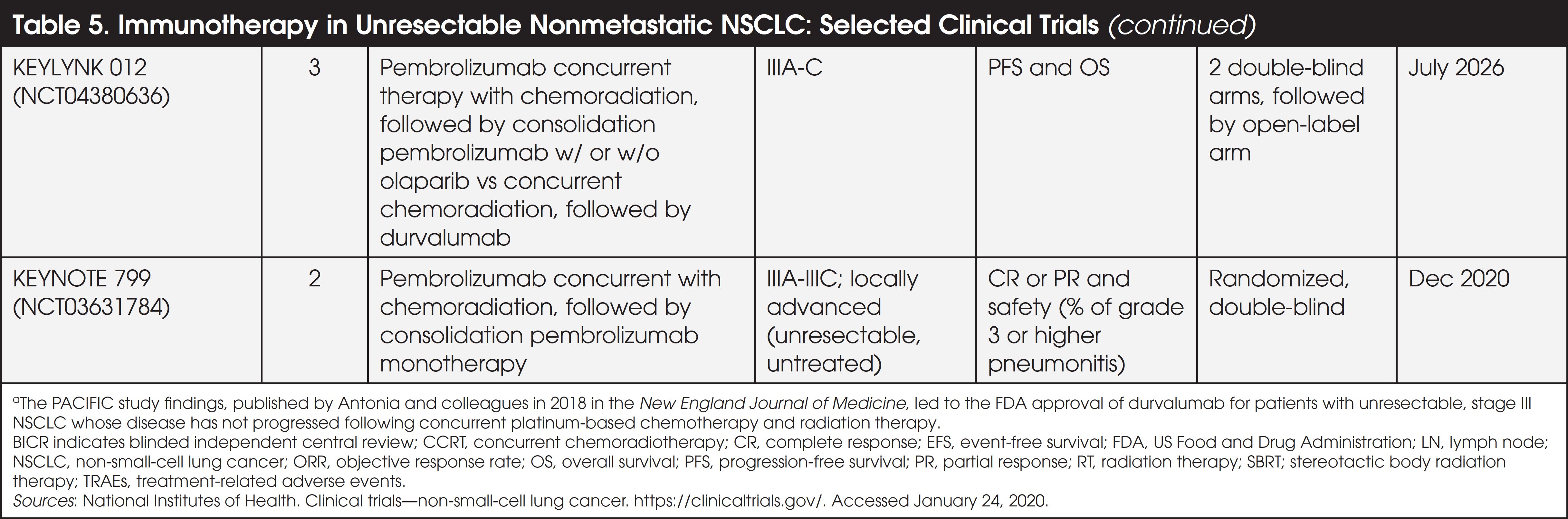
Currently, a number of clinical trials are investigating the potential role of immunotherapy—specifically the PD-1 and PD-L1 immune checkpoint inhibitors—in the treatment of resectable nonmetastatic NSCLC (Table 4)52-68 and unresectable nonmetastatic NSCLC (Table 5).69-81 These agents are being evaluated in various settings—neoadjuvant, adjuvant, and perioperative—in combination with or following chemotherapy, chemoradiation, RT, or SBRT. Findings from these studies may elucidate the potential role of immunotherapy in extending anti-tumor immune response to micrometastases, thereby reducing the risk of disease relapse or recurrence in patients with nonmetastatic NSCLC.82
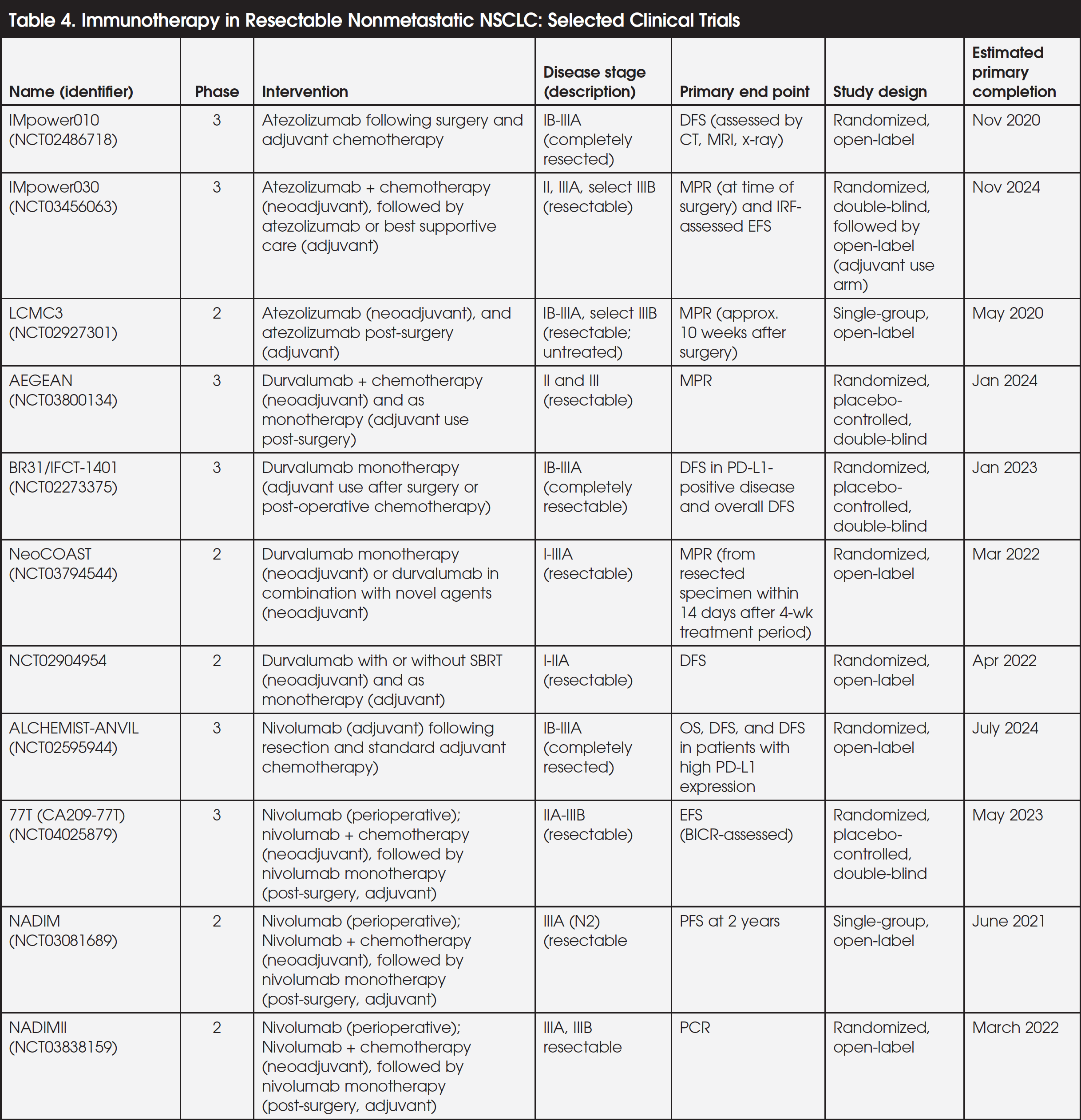
Durvalumab, a PD-L1 inhibitor, received FDA approval in 2018 to treat patients with unresectable stage III NSCLC whose disease had not progressed following concurrent platinum-based chemotherapy and RT, based on findings from the PACIFIC trial.30,31 Studies are being conducted on durvalumab in patients with resectable, nonmetastatic NSCLC, including the AEGEAN perioperative study, which is evaluating durvalumab concurrent with chemotherapy as neoadjuvant treatment and durvalumab monotherapy as post-surgical adjuvant treatment.55 Durvalumab is also being studied as monotherapy in the adjuvant setting after surgery or post-operative chemotherapy (BR31/IFCT-1401) in resectable NSCLC (Table 4).56 Other studies on durvalumab in resectable, nonmetastatic NSCLC include durvalumab in the neoadjuvant setting as monotherapy and in combination with novel agents (NeoCOAST),57 as well as the perioperative setting including neoadjuvant durvalumab with or without SBRT followed by adjuvant durvalumab monotherapy as monthly maintenance for 1 year following surgery (NCT02904954) (Table 4).58
In patients with unresectable, nonmetastatic NSCLC, durvalumab is being studied both as monotherapy and in combination with novel agents as consolidation treatment in several trials (PACIFIC, PACIFIC-4, PACIFIC-5, PACIFIC-6, COAST) (Table 5).69,71-73,75 Durvalumab is also being studied as monotherapy and as concurrent/consolidation treatment in the PACIFIC-2, EA5181, and DART trials (Table 5).70,74,76
Atezolizumab, a PD-L1 inhibitor, is being studied in patients with resectable, nonmetastatic NSCLC. These studies include the IMpower010 trial assessing the efficacy and safety of atezolizumab (16 cycles) compared with best supportive care following resection and adjuvant chemotherapy (Table 4).52 The perioperative IMpower030 study is evaluating atezolizumab plus chemotherapy in the neoadjuvant setting, followed by open-label adjuvant therapy with atezolizumab or best supportive care.53 Another perioperative trial (LCMC3) is evaluating the neoadjuvant use of atezolizumab, followed by adjuvant therapy (up to 1 year) following surgery in patients with resectable, nonmetastatic NSCLC who showed clinical benefit with neoadjuvant treatment (Table 4).54
Nivolumab, a PD-1 inhibitor, is being evaluated in the ALCHEMIST-ANVIL study as adjuvant therapy, following resection and chemotherapy, in resectable nonmetastatic NSCLC (Table 4).59 The perioperative 77T trial is assessing nivolumab plus chemotherapy in the neoadjuvant setting, followed by surgery and adjuvant treatment with nivolumab.60 Other trials evaluating nivolumab in the perioperative setting include the NADIM and NADIMII trials, which study nivolumab plus chemotherapy as neoadjuvant therapy, followed by nivolumab monotherapy as adjuvant treatment following surgery.61,62
Nivolumab is also being studied in the neoadjuvant setting as a concurrent treatment with chemotherapy in the CheckMate 816 trial (the nivolumab + ipilimumab, a cytotoxic T-lymphocyte antigen 4 [CTLA-4] inhibitor, study arm is closed and no longer enrolling patients).63 Another trial in the neoadjuvant setting (NEOSTAR) includes 4 treatment arms: nivolumab monotherapy; nivolumab in combination with ipilimumab; nivolumab in combination with chemotherapy; and nivolumab in combination with ipilimumab and chemotherapy (Table 4).64 Nivolumab, or nivolumab + ipilimumab, are also being studied as neoadjuvant therapy in the NA_00092076 trial.65 In unresectable, nonmetastatic NSCLC, nivolumab is being evaluated as concurrent/consolidation treatment in clinical trials (Table 5).77,78
The NICOLAS trial is investigating concurrent nivolumab and first-line chemoradiation, followed by nivolumab consolidation treatment, and the CheckMate 73L trial is investigating concurrent nivolumab with chemoradiation followed by either consolidation nivolumab monotherapy or consolidation nivolumab plus ipilimumab compared with definitive concurrent chemoradiation, followed by consolidation durvalumab (Table 5).77,78
Pembrolizumab, a PD-1 inhibitor, is being evaluated in patients with resectable, nonmetastatic NSCLC in several studies as follows: as adjuvant treatment versus placebo (KEYNOTE 091)66; and as a perioperative approach combined with chemotherapy in the neoadjuvant setting, followed by pembrolizumab monotherapy in the adjuvant setting (KEYNOTE 671) (Table 4).67 The perioperative TOP 1501 trial is also being conducted on the neoadjuvant use of pembrolizumab, followed by surgery and subsequent standard adjuvant chemotherapy with or without RT, followed by the adjuvant use of pembrolizumab (Table 4).68 In unresectable, nonmetastatic NSCLC, the efficacy and safety of SBRT with or without concurrent pembrolizumab are being investigated in the KEYNOTE 867 trial79; moreover, pembrolizumab with concurrent chemoradiation, followed by consolidation pembrolizumab with or without olaparib is being investigated in the KEYLYNK-012 trial (Table 5).80 The KEYNOTE 799 trial is assessing pembrolizumab plus concurrent chemoradiation, followed by consolidation pembrolizumab monotherapy.81
Ongoing clinical trials will inform the potential role of immunotherapy—alone, or in combination with other therapies for patients with nonmetastatic NSCLC—and the sequence, duration, and appropriate patients for these therapies.
References
- Duma N, Santana-Davila R, Molina JR. Non-small cell lung cancer: epidemiology, screening, diagnosis, and treatment. Mayo Clin Proc. 2019;94:1623-1640.
- SEER Cancer Stat Facts: Lung and Bronchus Cancer. National Cancer Institute. Bethesda, MD. https://seer.cancer.gov/statfacts/html/lungb.html. Accessed December 12, 2019.
- National Cancer Institute. Cancer screening. www.cancer.gov/about-cancer/screening. Accessed August 27, 2020.
- de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N Engl J Med. 2020;382:503-513.
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer V.6.2020. © National Comprehensive Cancer Network, Inc. 2020. All rights reserved. Accessed June 15, 2020. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
- National Cancer Institute. Cancer trends progress report—lung cancer screening. https://progressreport.cancer.gov/detection/lung_cancer. Accessed August 27, 2020.
- National Lung Screening Trial Research Team (NLSTRT), Aberle DR, Adams AM, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365:395-409.
- National Cancer Institute. Non-small cell lung cancer treatment (PDQ)—health professional version. Updated June 13, 2019. www.cancer.gov/types/lung/hp/non-small-cell-lung-treatment-pdq. Accessed January 14, 2020.
- Broderick SR. Faculty Perspectives transcript on file. STRATEGIX. March 2020.
- Kris MG, Gaspar LE, Chaft JE, et al. Adjuvant systemic therapy and adjuvant radiation therapy for Stage I to IIIA completely resected non-small-cell lung cancers: American Society of Clinical Oncology/Cancer Care Ontario Clinical Practice Guideline Update. J Clin Oncol. 2017;35:2960-2974.
- Postmus PE, Kerr KM, Oudkerk M, et al; for the ESMO Guidelines Committee. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(supple 4):iv1-iv21.
- Byron E, Pinder-Schenck M. Systemic and targeted therapies for early-stage lung cancer. Cancer Control. 2014;21:21-31.
- Detterbeck FD, Lewis SZ, Diekemper R, et al. Executive summary: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 suppl):7S-37S.
- Goldstraw P, Chansky K, Crowley J, et al; for the International Association for the Study of Lung Cancer International Staging and Prognostic Factors Committee Advisory Boards and Participating Institutions. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification of malignant tumors. J Thorac Oncol. 2016;11:39-51.
- Lou F, Sima CS, Rusch VW, et al. Differences in patterns of recurrence in early-stage versus locally advanced non-small cell lung cancer. Ann Thorac Surg. 2014;98:1755-1760.
- Lou F, Huang J, Sima CS, et al. Patterns of recurrence and second primary lung cancer in early-stage lung cancer survivors followed with routine computed tomography surveillance. J Thorac Cardiovasc Surg. 2013;145:75-81.
- American Cancer Society. Surgery for non-small cell lung cancer. Revised October 1, 2019. www.cancer.org/cancer/lung-cancer/treating-non-small-cell/surgery.html. Accessed February 28, 2019.
- Broderick SR, Grau-Sepulveda M, Kosinski AS, et al. The Society of Thoracic Surgeons composite score rating for pulmonary resection of lung cancer. Ann Thorac Surg. 2020;109:848-855.
- NSCLC Meta-Analysis Collaborative Group. Preoperative chemotherapy for non-small-cell lung cancer: a systematic review and meta-analysis of individual participant data. Lancet. 2014;383:1561-1571.
- Pignon JP, Tribodet H, Scagliotti GV, et al; for the LACE Collaborative Group. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26:3552-3559.
- Felip E, Rosell R, Maestre JA, et al; for the Spanish Lung Cancer Group. Preoperative chemotherapy plus surgery vs surgery plus adjuvant chemotherapy vs surgery alone in early-stage non-small-cell lung cancer. J Clin Oncol. 2010;28:3138-3145.
- American Cancer Society. Chemotherapy for non-small cell lung cancer. www.cancer.org/cancer/lung-cancer/treating-non-small-cell/chemotherapy.html. Accessed March 1, 2020.
- Hobbs CJ, Ko SJ, Paryani NN, et al. Stereotactic body radiotherapy for medically inoperable stage I-II non-small cell lung cancer: the Mayo Clinic experience. Mayo Clin Proc Innov Qual Outcomes. 2017;26:40-48.
- Timmerman R, Paulus R, Galvin J, et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA. 2010;303:1070-1076.
- Timmerman RD, Hu C, Michalski JM, et al. Long-term results of stereotactic body radiation therapy in medically inoperable stage I non-small cell lung cancer [letter]. JAMA Oncol. 2018;4:1287-1288.
- Palma DA, Nguyen TK, Louie AV, et al. Measuring the integration of stereotactic ablative radiotherapy plus surgery for early-stage non-small cell lung cancer. JAMA Oncol. 2019;5:681-688.
- Aupérin A, Le Péchoux C, Rolland E, et al; for the NSCLC Collaborative Group. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J Clin Oncol. 2010;28:2181-2190.
- Kang KY, Okoye CC, Patel RB, et al. Complications from stereotactic body radiotherapy for lung cancer. Cancers. 2015;7:981-1004.
- American Cancer Society. Treating non-small cell lung cancer. October 1, 2019. www.cancer.org/content/dam/CRC/PDF/Public/8706.00.pdf. Accessed February 28, 2020.
- Antonia SJ, Villegas A, Daniel D, et al; for the PACIFIC Investigators. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N Engl J Med. 2018;379:2342-2350.
- US Food and Drug Administration. FDA expands approval of Imfinzi to reduce the risk of non-small cell lung cancer progressing. February 16, 2018. www.fda.gov/news-events/press-announcements/fda-expands-approval-imfinzi-reduce-risk-non-small-cell-lung-cancer-progressing. Accessed June 3, 2020.
- Brahmer JR, Lacchetti C, Schneider BJ, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol. 2018;36:1714-1768.
- Centers for Disease Control and Prevention. US Cancer Statistics data visualizations tool—lung and bronchus cancer—trends; changes over time; annual rates of cancer deaths table, based on November 2018 submission data (1999-2016). June 2019. https://gis.cdc.gov/Cancer/USCS/DataViz.html. Accessed January 20, 2020.
- American Cancer Society. Lung Cancer Survival Rates. www.cancer.org/cancer/lung-cancer/detection-diagnosis-staging/survival-rates.html. Accessed August 31, 2020.
- SEER Training Modules. Five-year survival rates. https://training.seer.cancer.gov/lung/intro/survival.html. Accessed June 3, 2020.
- Gildea TR, DaCosta Byfield S, Hogarth DK, et al. A retrospective analysis of delays in the diagnosis of lung cancer and associated costs. Clinicoecon Outcomes Res. 2017;9:261-269.
- Chen Z, Fillmore CM, Hammerman PS, et al. Non-small-cell lung cancers: a heterogeneous set of diseases (erratum appears in Nat Rev Cancer. 2015;15:247). Nat Rev Cancer. 2014;14:535-546.
- ASCO-ESMO consensus statement on quality cancer care. J Clin Oncol. 2006;24:3498-3499. Epub June 2, 2006. www.ncbi.nlm.nih.gov/pubmed/16751437.
- Forde P. Faculty Perspectives transcript on file. STRATEGIX. March 2020.
- Schneider BJ, Ismaila N, Aerts J, et al. Lung cancer surveillance after definitive curative-intent therapy: ASCO guideline. J Clin Oncol. 2019;37:1-16.
- Huber RM, De Ruysscher D, Hoffmann H, et al. Interdisciplinary multimodality management of stage III nonsmall cell lung cancer. Eur Respir Rev. 2019;28(152). Epub June 30, 2019.
- Friedman EL, Kruklitis RJ, Patson BJ, et al. Effectiveness of a thoracic multidisciplinary clinic in the treatment of stage III non-small-cell lung cancer. J Multidiscip Healthc. 2016;9:267-274.
- Bilfinger TV, Albano D, Perwaiz M, et al. Survival outcomes among lung cancer patients treated using a multidisciplinary team approach. Clin Lung Cancer. 2018;19:346-351.
- Kehl KL, Landrum MB, Kahn KL, et al. Tumor board participation among physicians caring for patients with lung or colorectal cancer. J Oncol Pract. 2015;11:e267-278.
- Soukup T, Lamb BW, Arora S, et al. Successful strategies in implementing a multidisciplinary team working in the care of patients with cancer: an overview and synthesis of the available literature. J Multidiscip Healthc. 2018;11:49-61.
- Horner K, Ludman EJ, McCorkle R, et al. An oncology nurse navigator program designed to eliminate gaps in early cancer care. Clin J Oncol Nurs. 2013;17:43-48.
- Oncology Nursing Society (ONS). Role of the oncology nurse navigator throughout the cancer trajectory. March 2018. www.ons.org/make-difference/advocacy-and-policy/position-statements/ONN. Accessed January 22, 2020.
- Dobrea L, Gansauer LJ. The navigator’s role in supporting clinical trials. J Oncol Navig Surviv. 2018;9:324-325.
- Wagner EH, Ludman EJ, Aiello Bowles EJ, et al. Nurse navigators in early cancer care: a randomized, controlled trial. J Clin Oncol. 2014;32:12-18.
- Peckham J, Mott-Coles S. Interprofessional lung cancer tumor board: the role of the oncology nurse navigator in improving adherence to national guidelines and streamlining patient care. Clin J Oncol Nurs. 2018;22:656-662.
- Foster CC, Sher DJ, Rusthoven CG, et al. Overall survival according to immunotherapy and radiation treatment for metastatic non-small-cell lung cancer: A National Cancer Database analysis. Radiat Oncol. 2019;14:18.
- National Institutes of Health. Study to assess safety and efficacy of atezolizumab (MPDL3280A) compared to best supportive care following chemotherapy in patients with lung cancer (IMpower010). NCT02486718. https://clinicaltrials.gov/ct2/show/NCT02486718. Accessed January 24, 2020.
- National Institutes of Health. A study of neoadjuvant atezolizumab plus chemotherapy plus chemotherapy in patients with resectable stage III, IIIA, or select IIIB non-small cell lung cancer (IMpower030). NCT03456063. https://clinicaltrials.gov/ct2/show/NCT03456063. Accessed January 24, 2020.
- National Institutes of Health. A study of atezolizumab as neoadjuvant therapy in resectable non-small cell lung cancer (NSCLC)—Lung Cancer Mutation Consortium (LCMC3). NCT02927301. https://clinicaltrials.gov/ct2/show/NCT02927301. Accessed January 23, 2020.
- National Institutes of Health. A study of neoadjuvant/adjuvant durvalumab for the treatment of patients with resectable non-small cell lung cancer (AEGEAN). NCT03800134. https://clinicaltrials.gov/ct2/show/NCT03800134. Accessed January 23, 2020.
- National Institutes of Health. Double-blind, placebo-controlled study of adjuvant MEDI14736 in completely resected NSCLC (BR 31; also known as IFCT-1401). NCT02273375. https://clinicaltrials.gov/ct2/show/NCT02273375. Accessed January 23, 2020.
- National Institutes of Health. Neoadjuvant durvalumab alone or in combination with novel agents in resectable non-small cell lung cancer (NeoCOAST). NCT03794544. https://clinicaltrials.gov/ct2/show/NCT03794544. Accessed January 30, 2020.
- National Institutes of Health. Durvalumab (MEDI14736) with or without SBRT in clinical stage I, II and IIIA non-small cell lung cancer. NCT02904954. https://clinicaltrials.gov/ct2/show/NCT02904954. Accessed January 24, 2020.
- National Institutes of Health. Nivolumab after surgery and chemotherapy in treating patients with stage IB-IIIA non-small cell lung cancer (an ALCHEMIST Treatment Trial) (ANVIL). NCT02595944. www.clinicaltrials.gov/ct2/show/NCT02595944. Accessed January 14, 2020.
- National Institutes of Health. A study of neoadjuvant chemotherapy plus nivolumab versus neoadjuvant chemotherapy plus placebo, followed by surgical removal and adjuvant treatment with nivolumab or placebo for participants with surgically removable early stage non-small cell lung cancer. NCT04025879. https://clinicaltrials.gov/ct2/show/NCT04025879. Accessed January 16, 2020.
- National Institutes of Health. Neo-adjuvant immunotherapy with nivolumab for non-small cell lung cancer patients (NADIM). NCT03081689. https://clinicaltrials.gov/ct2/show/NCT03081689. Accessed January 30, 2020.
- National Institutes of Health. NADIM II: neoadjuvant immunotherapy (NADIMII). NCT03838159. https://clinicaltrials.gov/ct2/show/NCT03838159. Accessed January 30, 2020.
- National Institutes of Health. A neoadjuvant study of nivolumab plus ipilimumab or nivolumab plus chemotherapy versus chemotherapy alone in early stage non-small cell lung cancer (NSCLC) (CheckMate 816). NCT02998528. https://clinicaltrials.gov/ct2/show/NCT02998528. Accessed January 16, 2020.
- National Institutes of Health. Nivolumab with or without ipilimumab or chemotherapy in treating patients with previously untreated stage I-IIIA non-small cell lung cancer (NEOSTAR trial). NCT03158129. https://clinicaltrials.gov/ct2/show/NCT03158129. Accessed January 23, 2020.
- National Institutes of Health. Neoadjuvant nivolumab, or nivolumab in combination with ipilimumab, in resectable NSCLC (NA_00092076). NCT02259621. https://clinicaltrials.gov/ct2/show/NCT02259621. Accessed January 23, 2020.
- National Institutes of Health. Study of pembrolizumab (MK-3475) vs placebo for participants with non-small cell lung cancer after resection with or without standard adjuvant therapy (KEYNOTE-091). NCT02504372. https://clinicaltrials.gov/ct2/show/NCT02504372. Accessed January 23, 2020.
- National Institutes of Health. Efficacy and safety of pembrolizumab (MK-3475) with platinum doublet chemotherapy as neoadjuvant/adjuvant therapy for participants with resectable stage II, IIIA, and resectable IIIB (T3-4N2) non-small cell lung cancer (KEYNOTE-671). NCT03425643. https://clinicaltrials.gov/ct2/show/NCT03425643. Accessed January 23, 2020.
- National Institutes of Health. Neoadjuvant pembrolizumab (TOP 1501). NCT028118920. https://clinicaltrials.gov/ct2/show/NCT02818920. Accessed January 24, 2020.
- National Institutes of Health. A global study to assess the effects of MEDI4736 following concurrent chemoradiation in patients with stage III unresectable non-small cell lung cancer (PACIFIC). NCT02125461. https://clinicaltrials.gov/ct2/show/NCT02125461. Accessed January 23, 2020.
- National Institutes of Health. Study of durvalumab given with chemoradiation therapy in patients with unresectable non-small cell lung cancer (PACIFIC-2). NCT03519971. https://clinicaltrials.gov/ct2/show/NCT03519971. Accessed January 30, 2020.
- National Institutes of Health. Durvalumab vs placebo following stereotactic body radiation therapy in early-stage non-small-cell lung cancer patients (PACIFIC-4). NCT03833154. https://clinicaltrials.gov/ct2/show/NCT03833154. Accessed January 23, 2020.
- National Institutes of Health. A study of durvalumab as consolidation therapy in non-small cell lung cancer patients (PACIFIC-5). NCT03706690. https://clinicaltrials.gov/ct2/show/NCT03706690. Accessed January 23, 2020.
- National Institutes of Health. A study to determine safety of durvalumab after sequential chemo radiation in patients with unresectable stage III non-small cell lung cancer (PACIFIC-6). NCT03693300. https://clinicaltrials.gov/ct2/show/NCT03693300. Accessed June 8, 2020.
- National Institutes of Health. Testing the addition of an antibody to standard chemoradiation followed by the antibody for one year to standard chemoradiation followed by one year of the antibody in patients with unresectable stage III non-small cell lung cancer (EA5181 [NCI-2019-06124]). NCT04092283. https://clinicaltrials.gov/ct2/show/NCT04092283. Accessed January 30, 2020.
- National Institutes of Health. Durvalumab alone or in combination with novel agents in subjects with NSCLC (COAST). NCT03822351. https://clinicaltrials.gov/ct2/show/NCT03822351. Accessed January 30, 2020.
- National Institutes of Health. Determining whether durvalumab in combination with radiation therapy can prevent the progression of non-small cell lung cancer (DART). NCT03999710. https://clinicaltrials.gov/ct2/show/NCT03999710. Accessed January 24, 2020.
- National Institutes of Health. Nivolumab combination with standard first-line chemotherapy and radiotherapy in locally advanced Stage IIIA/B non-small cell lung carcinoma (NICOLAS). NCT02434081. https://clinicaltrials.gov/ct2/show/NCT02434081. Accessed January 30, 2020.
- National Institutes of Health. A study of nivolumab and ipilimumab in untreated patients with stage 3 NSCLC that is unable or not planned to be removed by surgery (CheckMate73L). NCT04026412. https://clinicaltrials.gov/ct2/show/NCT04026412. Accessed January 16, 2020.
- National Institutes of Health. Efficacy and safety study of stereotactic body radiotherapy (SBRT) with or without pembrolizumab (MK-3475) in adults with medically inoperable stage I or IIA non-small cell lung cancer (NSCLC) (KEYNOTE-867). NCT03924869. https://clinicaltrials.gov/ct2/show/NCT03924869. Accessed January 23, 2020.
- National Institutes of Health. Study of pembrolizumab with concurrent chemoradiation therapy followed by pembrolizumab with or without olaparib in stage III non-small cell lung cancer (NSCLC) (MK-7339-012/KEYLYNK-012). NCT04380636. https://clinicaltrials.gov/ct2/show/NCT04380636. Accessed June 8, 2020.
- National Institutes of Health. A trial of pembrolizumab in combination with chemotherapy and radiotherapy in stage III NSCLC (KEYNOTE-799, MK-3475-799). NCT03631784. https://clinicaltrials.gov/ct2/show/NCT03631784. Accessed January 23, 2020.
- Owen D, Chaft JE. Immunotherapy in surgically resectable non-small cell lung cancer. J Thorac Dis. 2018;10(suppl 3):S404-5411.