
This research was presented, in part, as a poster at the 2022 ASCO Quality Care Symposium and online-only as an abstract at the 2023 ASCO Annual Meeting. This manuscript contains original material that is not already available elsewhere. The Association of Cancer Care Centers’ Financial Advocacy Services Guidelines report, which resulted from the research detailed in this manuscript, was released publicly online March 8, 2023, and is available at www.accc-cancer.org/home/learn/financial-advocacy/guidelines.
Introduction: Financial advocacy interventions (also known as financial navigation) can potentially address the financial distress that many people with cancer experience. Yet the financial advocacy services offered to patients continue to vary. Standardization is necessary for equitable delivery and effective evaluation of financial advocacy interventions.
Methods: The Financial Advocacy Services Guidelines were developed through a Delphi study with 49 experts. A literature review and qualitative input from panelists informed a list of 44 potential guidelines. Panelists completed 2 rounds of anonymous voting to reach consensus (≥75% agreement) on final guidelines.
Results: Panelists reached consensus on 43 final guidelines across 3 domains and 8 subdomains: (1) financial advocacy services and functions, (2) program management functions, and (3) partner engagement functions.
Conclusion: This study produced consensus-based guidelines through a rigorous and engaged process. To reduce the impacts of financial distress on patients with cancer and their families, healthcare organizations should adhere to as many guidelines as feasible. Given their role in distress screening and needs navigation, navigators play an important role in implementing and delivering these services.
Rapid innovations in diagnostics and treatments and an increasingly complex health insurance landscape have resulted in increased costs for people with cancer, their families, and healthcare systems alike. Evidence from a systematic review of 25 research studies suggests that at least half of people with cancer experience financial distress—a common adverse effect of costly cancer care.1 Tucker-Seeley et al2 found that 29% of patients with a terminal cancer diagnosis reported depleting all or most of their savings because of their illness. Ramsey et al3 reported that patients with cancer were 2.65 times more likely to go bankrupt than people without cancer.
Financial distress negatively impacts treatment outcomes and quality of life for patients with cancer and their families.4 Financial distress has been associated with increased mortality.3,5 In addition to paying for costly care, patients in active anticancer treatment often suffer a loss of income from the inability to work. Furthermore, those who cannot afford direct (eg, co-pays) or indirect (eg, transportation, special dietary expenses) treatment-related costs may choose to borrow money or delay paying other bills to cover their medical expenses, or they may reduce, delay, or avoid their anticancer treatment altogether.1,4,6
Healthcare organizations have begun to treat and potentially prevent financial distress among patients with cancer by providing services that address its common causes. Financial advocacy (also known as financial navigation) is a promising intervention to address financial distress, benefiting both people with cancer and the healthcare organization serving them.6 Key components of a standardized and multidisciplinary approach to addressing financial distress include screening patients to assess risk and providing financial education, counseling, and/or navigation as needed.6 Doherty et al7 identified 3 core functions of financial advocacy programs: (1) helping patients prepare for their out-of-pocket (OOP) costs, (2) optimizing patients’ health insurance, and (3) maximizing any available financial assistance for patients’ medical and nonmedical expenses.
It is evident that there is no single definition for “financial advocacy” and no standard intervention(s) used across the board. Increasingly, pilot studies and clinical trials are using different combinations of services and evaluating their impacts on patient-reported implementation, financial issues, and clinical outcomes (eg, satisfaction, feasibility, health insurance literacy, financial distress, quality of life, and cost-related nonadherence).8-12 For example, Wheeler et al qualitatively examined their Lessening the Impact of Financial Toxicity (LIFT) intervention and identified 6 core functions believed to make LIFT effective and 5 core functions believed to facilitate LIFT’s implementation. Their randomized controlled trial is ongoing to examine LIFT’s outcomes and impact, but pilot data showed reductions in patient OOP costs and financial distress.10,13,14 Chelsea et al shared preliminary results showing that implementing financial distress screening was feasible and increased identification of patients and referrals to navigation support.15 Henrikson et al report that their Cancer Financial Experience (CAFÉ) financial navigation program is acceptable and helpful to patients.16,17 The 4-session virtually delivered health insurance navigation intervention by Kirchoff et al improved several patient insurance knowledge metrics and perceived stress more so than usual navigation.18
A review by Offodile et al19 describes several different models for delivering financial advocacy services, including integrated delivery within the cancer program, remote delivery by national nonprofit advocacy groups or community-based organizations, and use of commercial technology or app-based solutions. Despite the various emerging models, a 2016 Association of Cancer Care Centers (ACCC) survey showed that only 39% of respondents’ organizations routinely offered financial advocacy services, such as meeting with all patients to discuss the cost of care.20 Further, while most of the National Cancer Institute Community Oncology Research Program’s members report offering financial navigation services,21 only half have dedicated financial advocates, and those serving racially and ethnically diverse and low-income communities were less likely to screen for financial distress and provide financial advocacy.22
As costs rise, leaders in the field have been increasingly vocal about the need for more research on mitigating patients’ financial distress and standardizing and institutionalizing the use of financial advocacy services in cancer care delivery.6,19 A critical step toward reaching this goal is defining guidelines, which can facilitate greater consistency in research to understand the effectiveness and optimal implementation of financial advocacy programs and services—ultimately helping administrators and multidisciplinary cancer care teams build evidence-based programs to improve care for people with cancer. Therefore, the purpose of this study was to develop consensus-based financial advocacy services guidelines.
Methods
Given the lack of practice guidelines or a standardized definition of core financial advocacy services, ACCC’s Financial Advocacy Network leadership convened a task force to design a Delphi study. The task force comprised financial advocacy experts representing navigation, nursing, social work, research, patient advocacy, and administration.
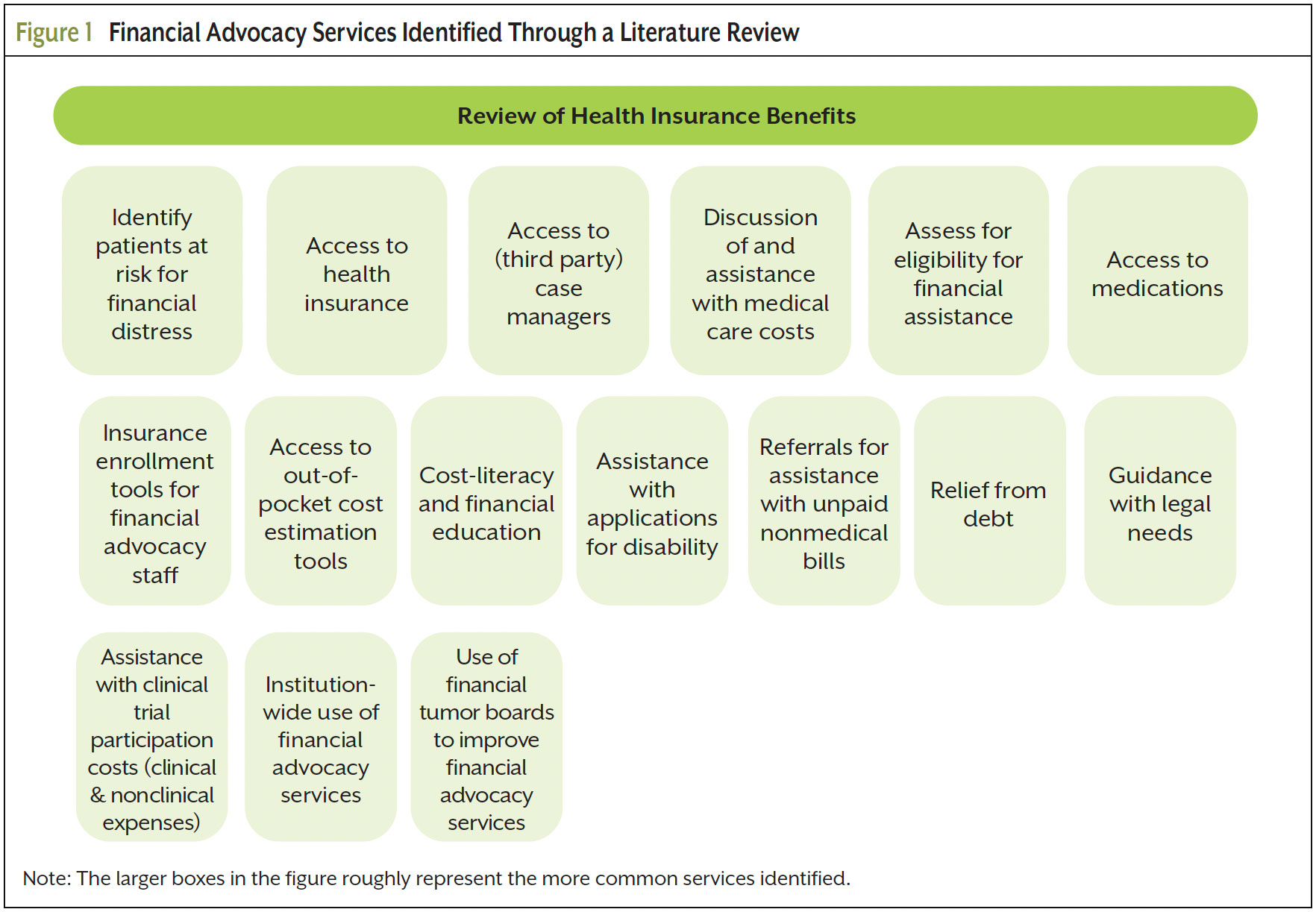
The task force conducted a literature review limited to articles published between January 2016 and December 2021 to capture current evidence. PubMed and Google searches were conducted using the terms “financial advocacy or financial navigation or financial toxicity” and “cancer or oncology.” Articles and studies conducted or describing practices outside the United States were excluded. A total of 55 articles were identified: 21 original research articles, 16 commentaries, 14 reviews, 2 editorials, 1 blog post, and 1 position paper. Figure 1 depicts the financial advocacy services discussed in these articles.
The task force initially drafted 42 potential guidelines related to services identified in the literature review as well as health insurance, patient assistance services, and financial advocacy team characteristics outlined in a 2018 report from ACCC’s Financial Advocacy Network.23
The task force defined qualifying criteria for the Delphi study and recruited a panel of experts with extensive knowledge of oncology financial advocacy programs and the populations they serve. Experts gained this knowledge through employment at a cancer center delivering financial navigation services, advocacy work, academic research, and/or personal experience with receiving these services. The task force solicited panel nominations by disseminating recruitment information through professional networks. The task force received 113 panel nominations and extended invitations to 50 experts that reflect diversity of practice setting, geography, demographic background, and experience.
Panelists’ identities remained anonymous throughout. A questionnaire was distributed using Qualtrics for each round. In the first round, panelists received an overview document that outlined the Delphi process and goals, and panelists were asked to respond to 3 open-ended questions that encouraged them to brainstorm best practices for oncology financial advocacy programs. The task force subsequently sorted and collapsed the responses into an affinity diagram to identify potential edits and/or additions to the 42 drafted guidelines.
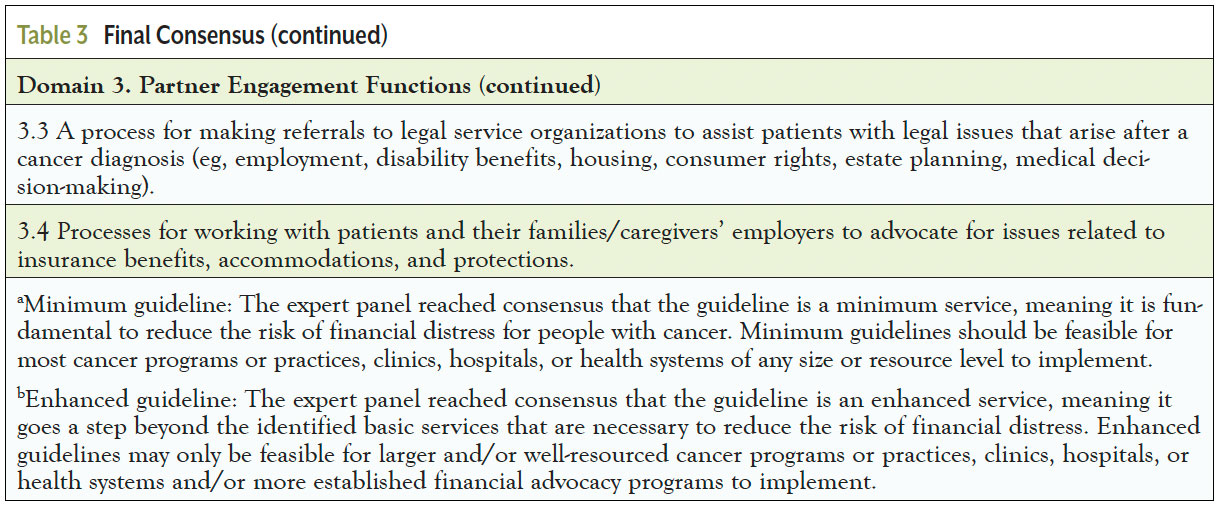
In Rounds 2 and 3, panelists were asked to assess each proposed guideline. Panelists rated each guideline as either “a minimum guideline” or “an enhanced guideline” to provide further expert consensus-based guidance around “must-have” versus “nice-to-have” financial advocacy services. Panelists also had an option to respond that a proposed guideline should not be a guideline or that they were not sure. The definitions provided to panelists are as follows:
- Minimum guideline: A fundamental service or function that is necessary to reduce risk of financial distress for patients with cancer. Minimum guidelines should be feasible for cancer programs, hospitals, or health systems of any size/resource level to implement
- Enhanced guideline: Important financial advocacy services and functions that go a step beyond basic services to proactively prevent financial distress and improve patient choice and quality of life. Enhanced guidelines may only be feasible for larger or well-resourced organizations or more established financial advocacy programs to implement
Panel responses were totaled after each questionnaire, and consensus was set a priori at 75% agreement. Any guidelines where at least 75% of panelists responded either “should be a minimum guideline” or “should be an enhanced guideline” were retained. In Round 2, panelists provided comments on each proposed guideline to help with wordsmithing. Guidelines that did not reach consensus were dropped or substantially revised. Between rounds 2 and 3, the task force developed a document to aggregate panelists’ responses and revise the proposed guidelines based on feedback. Panelists received this document for review prior to completing the final questionnaire. In Round 3, panelists provided general comments on the proposed guidelines.
Results
Delphi Panel
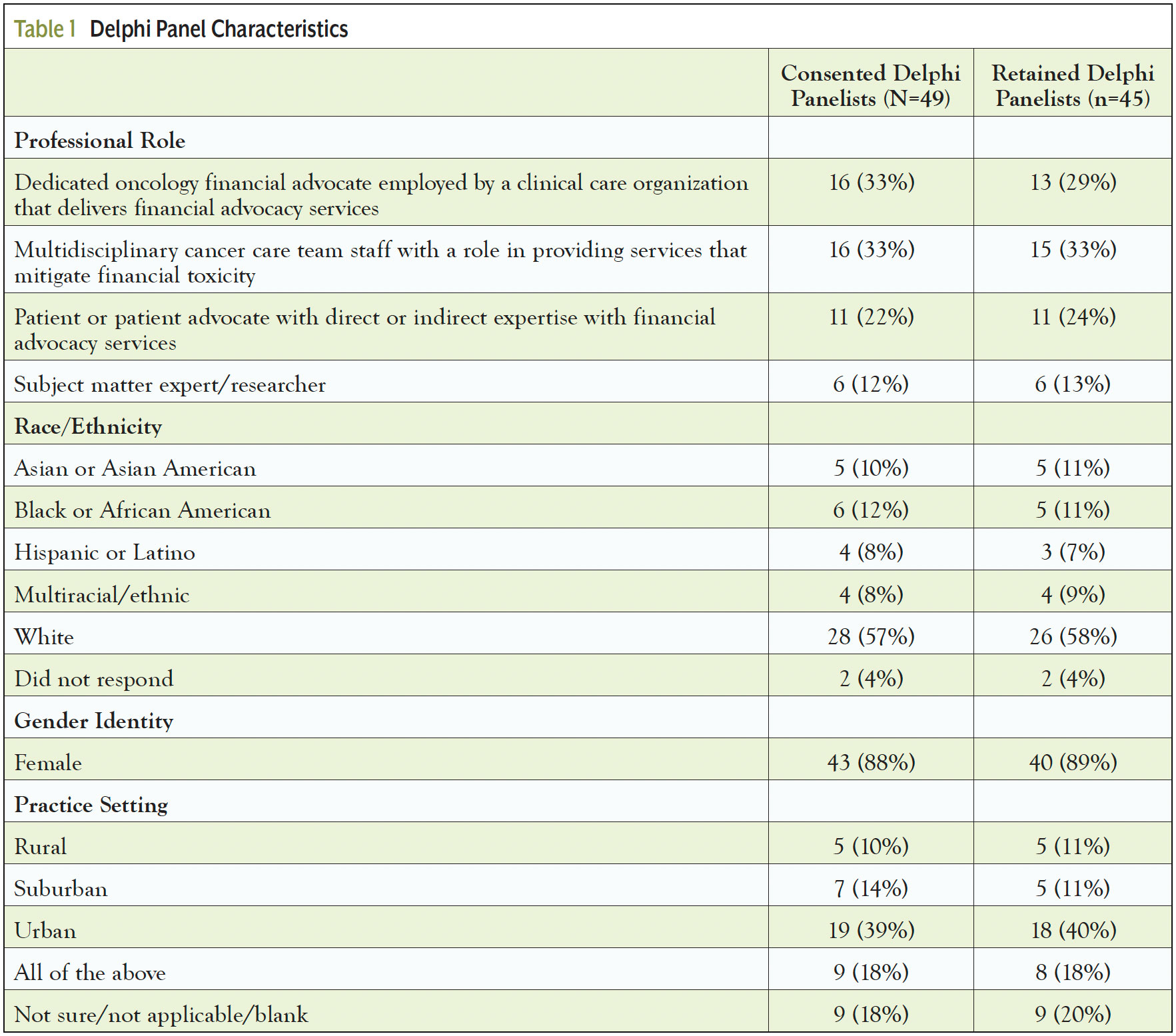
Of the 50 invited panelists, 49 agreed to participate; there was a 92% response rate (N=45), and 98% retention rate across the 3 rounds. Panelists who were financial or patient advocates and subject matter experts had a median of 6 to 10 years of professional experience; those who were multidisciplinary cancer care team members had a median of 11 to 15 years of professional experience. Table 1 illustrates the panel’s characteristics.
Round 1
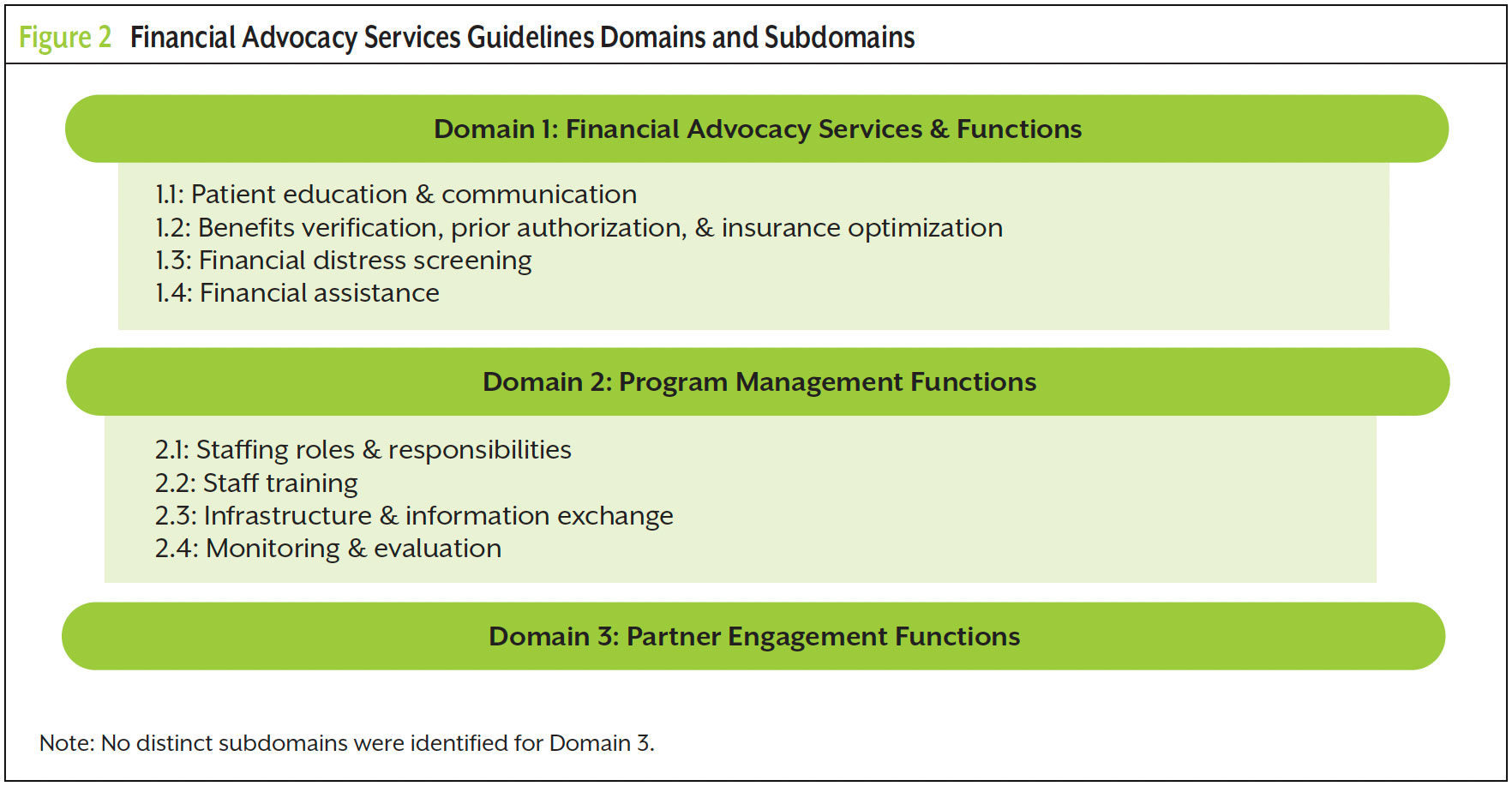
Panelists provided rich qualitative responses detailing many important activities, services, and infrastructure necessary for program success. Affinity sorting produced 3 major guideline domains and 8 subdomains (Figure 2). When comparing the affinity diagram from Round 1 with the 42 guidelines initially drafted by the task force, 2 gaps were identified that required drafting additional guidelines, and minor adjustments were made to the other guidelines. Round 1 data also provided much-needed context for how the guidelines should be used in practice, which is detailed fully in the final ACCC report.24
Round 2
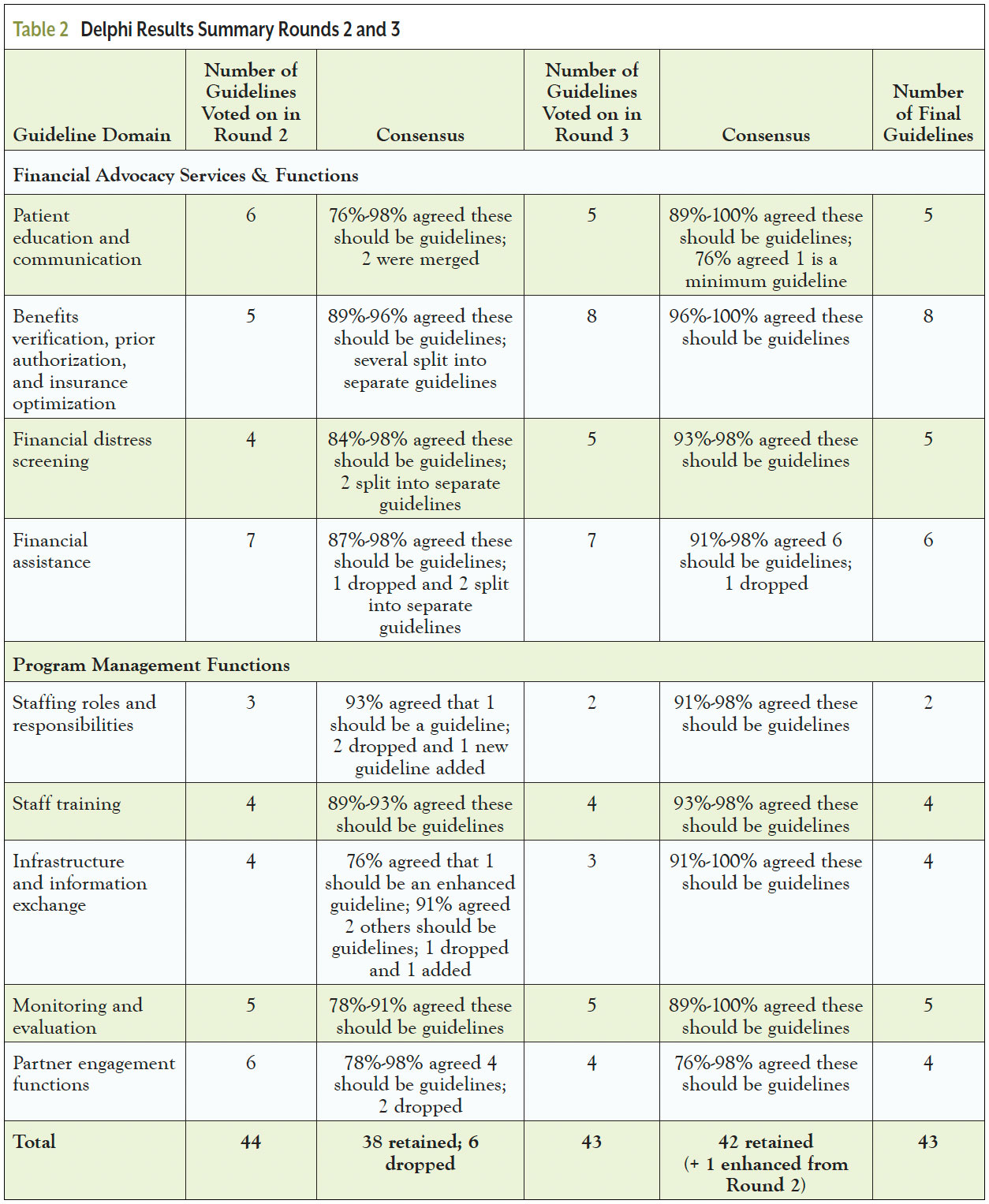
Table 2 summarizes the panel’s voting results. Of the 44 proposed guidelines, 38 reached consensus that they should be guidelines. Six were dropped due to a lack of consensus or feedback from panelists. Based on panel comments, the 38 guidelines were revised and/or split into their own statements because they represented distinct activities resulting in 43 guidelines for Round 3 voting. Comments in this round focused on removing any services that should be universal across a healthcare organization and not limited to financial advocacy programs; streamlining and eliminating redundancies; ensuring accuracy, clarity, and specificity of language; and considering feasibility and ideal evidence-informed practices within resource constraints.
Round 3
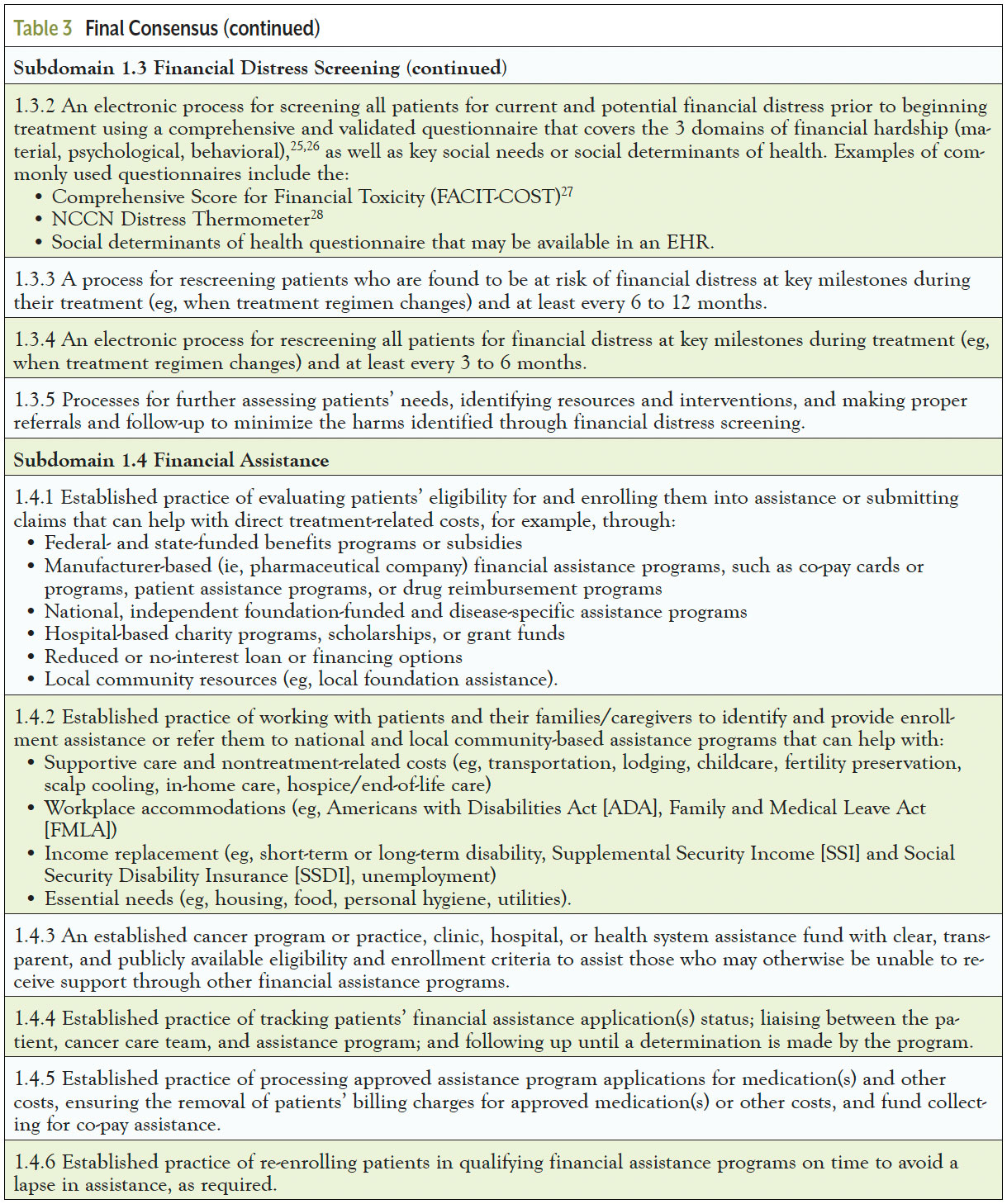
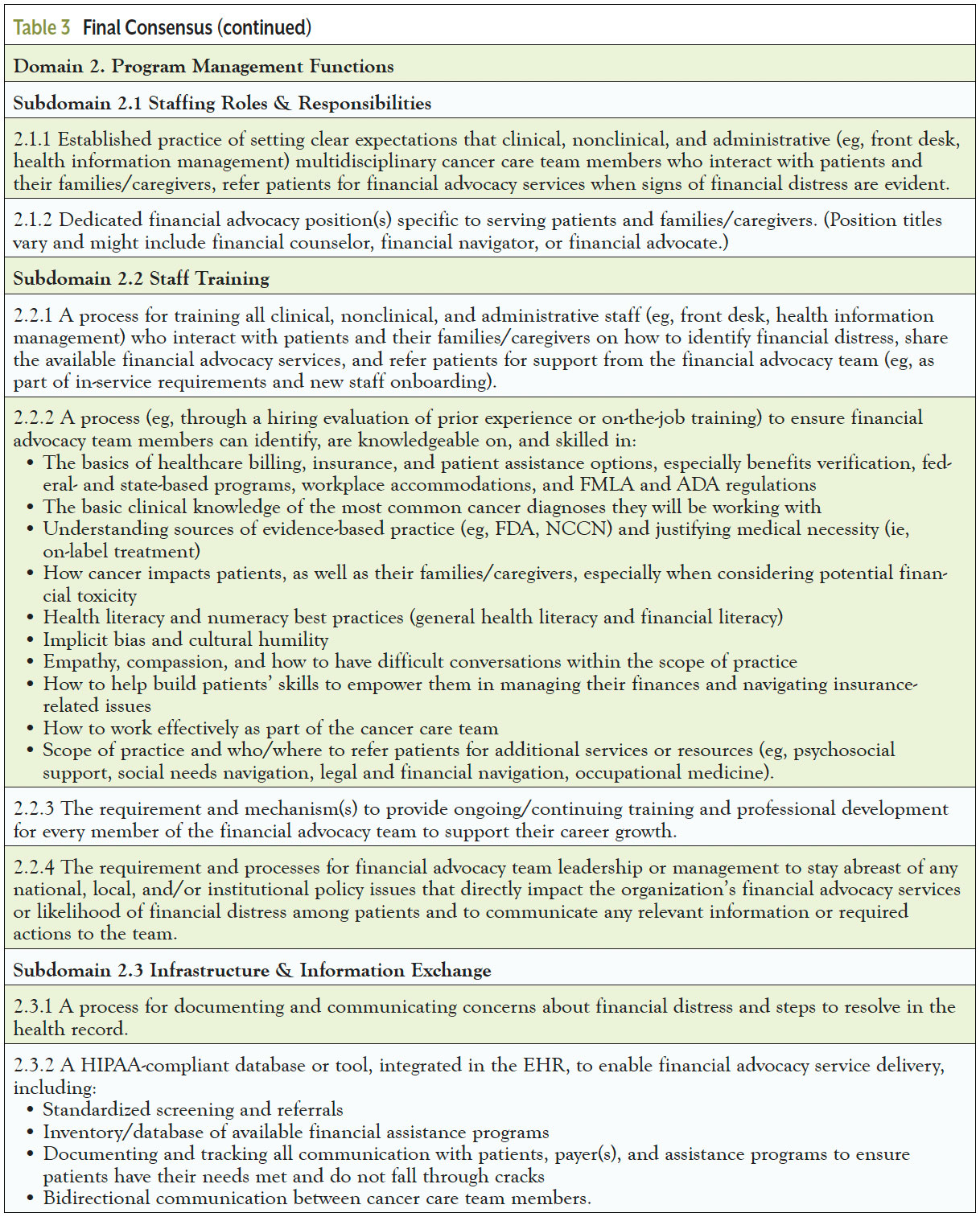
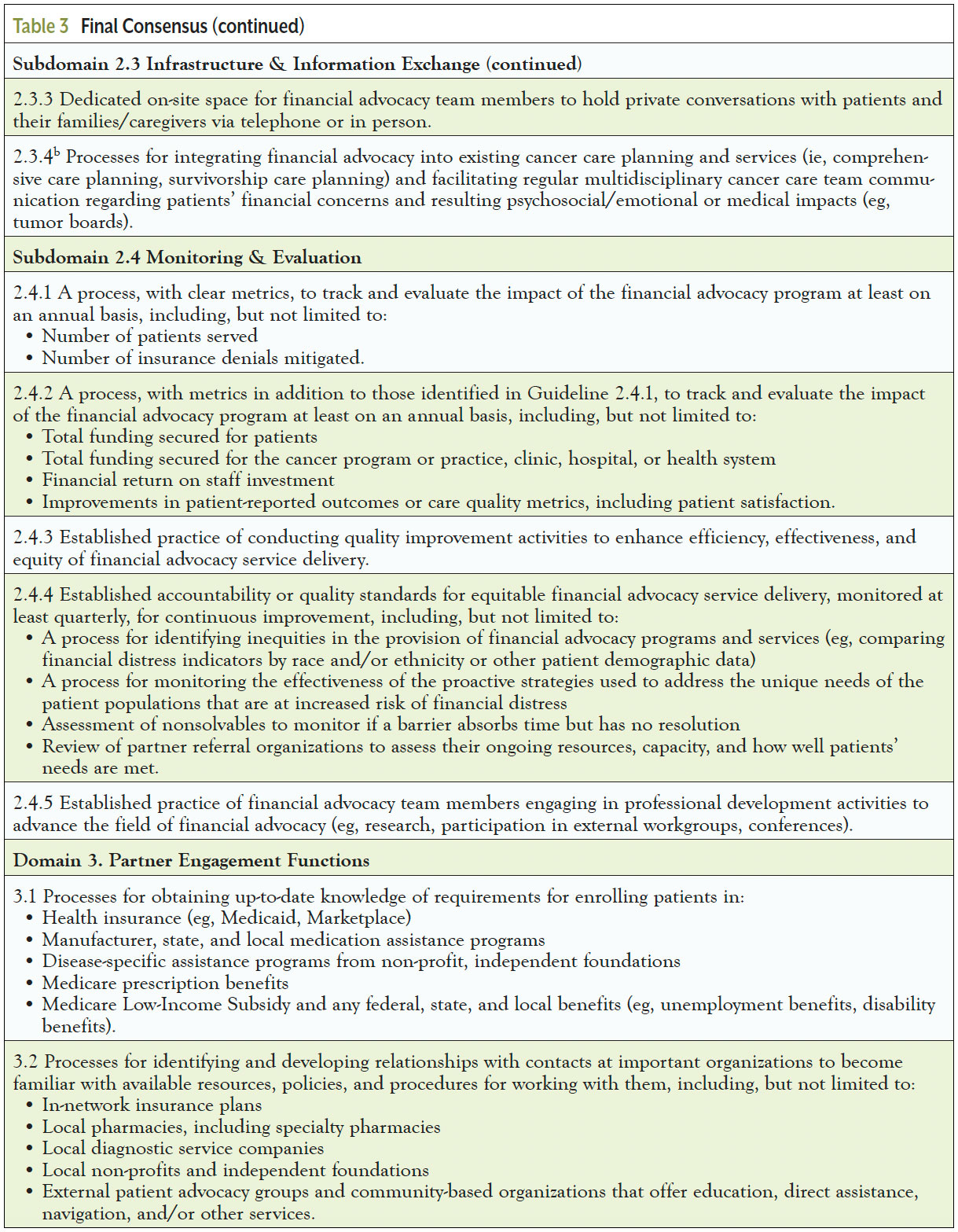
In the third round, 42 of the 43 proposed guidelines reached consensus that they should be final guidelines. One proposed guideline was dropped due to a lack of consensus. Panelists’ comments focused largely on implementation considerations, so the task force made only minor edits to the guidelines’ language for consistency and clarity. Including the one enhanced guideline agreed on in Round 2, the task force published 43 financial advocacy services guidelines (Table 3).
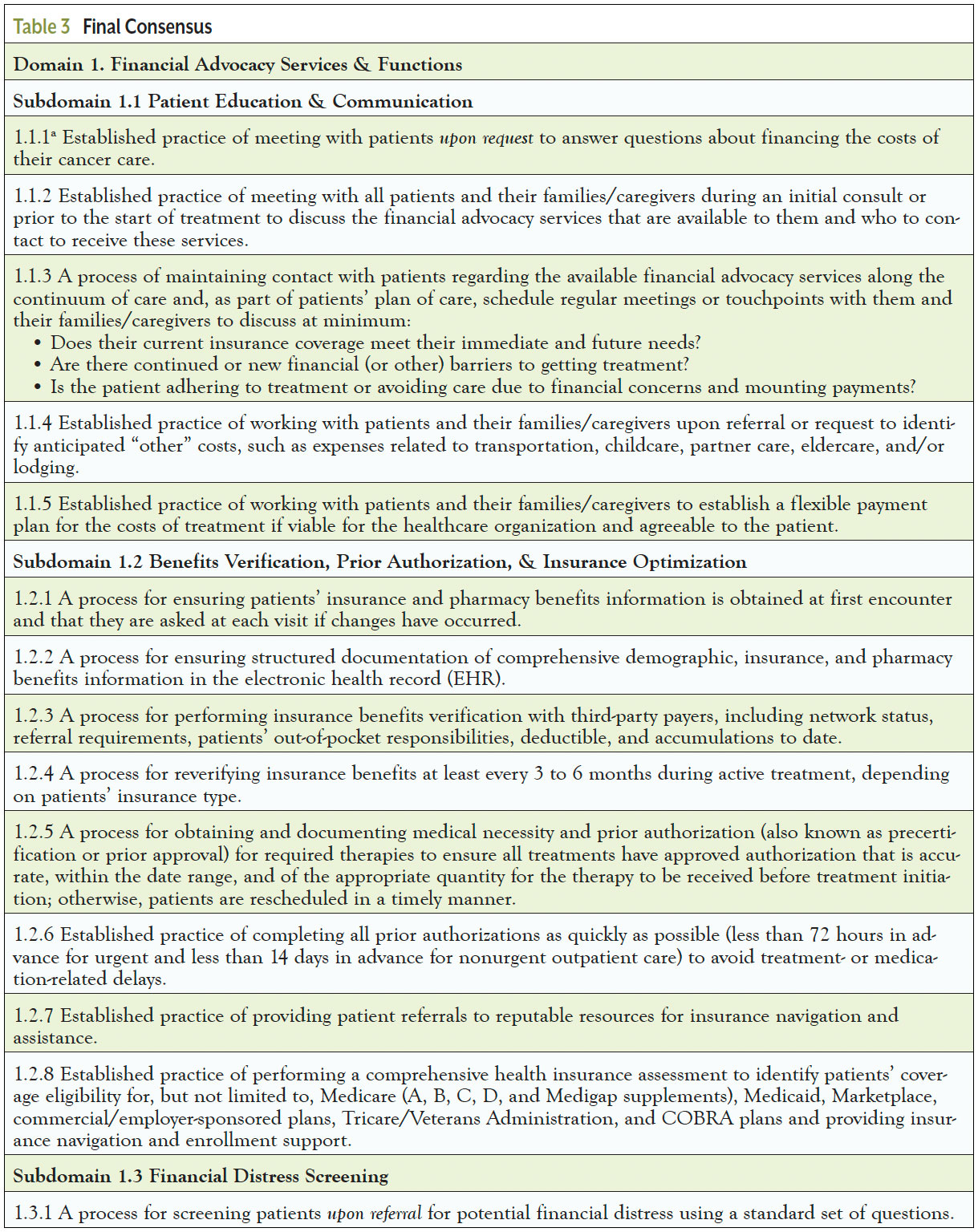
Minimum Versus Enhanced Guideline Designations
One guideline (1.1.1) reached consensus that it should be a minimum guideline, and one (2.3.4) reached consensus that it should be an enhanced guideline.
Discussion
Strong Consensus for Guidelines and Implications for Policy
The Delphi panel results show strong agreement among the multidisciplinary experts on the 43 Financial Advocacy Services Guidelines. Healthcare organizations can look to the Guidelines when setting institutional policies addressing costs of care and financial distress. Individuals with a policy role in healthcare financing and addressing social needs can look to the Guidelines as a framework for where system-level changes are needed to improve affordability and proactively reduce financial distress.
Across the 3 rounds, panelists largely agreed on most of the guidelines included in the financial advocacy services and functions domain. Their comments reflected patient-centeredness and urgency for addressing the risks and consequences of financial distress among patients with cancer. The resulting guidelines detail recommended services for patients and their caregivers to mitigate financial distress following a cancer diagnosis. These include supporting patient education and communication, completing financial distress screening, providing benefits verification and insurance optimization, and providing financial assistance. Panelists acknowledged that adherence to these guidelines would depend on available organizational resources. For example, panelists could not reach consensus on the timing and frequency of financial distress screening and rescreening, use of technology solutions to support service delivery and documentation, or feasibility to provide the guidelines’ services to all patients or just a higher-risk subset based on patient request or care team referral.
The Guidelines also include a program management functions domain, which includes the processes that underpin a healthcare organization’s ability to deliver a full scope of financial advocacy services. These include staffing roles and responsibilities, training, infrastructure and information exchange, and program monitoring and evaluation. Panelists recognized the importance of these functions and that organizations may implement them in different ways, leveraging their available resources and staff. They also recognized the important role navigators play in delivery of these services. What matters most is that the multidisciplinary cancer care team understands financial distress, strategies for mitigation, and available processes for addressing patients’ identified needs. This aligns with other financial advocates’ opinions about current barriers and proposed solutions.29
The final domain in the Guidelines includes partner engagement functions. These guidelines highlight the importance of general awareness of and connections with partners, networks, and policies to effectively deliver the financial advocacy services outlined. This knowledge foundation includes information about the insurance and financial assistance programs that are available locally and nationally, as well as building relationships with external organizations to enable information sharing and patient referrals.
Minimum Versus Enhanced Guideline Designations
While reaching consensus on 43 guidelines, the panelists only reached ≥75% agreement for the minimum/enhanced designation for 2 guidelines. Panelists recognized the minimum guideline (1.1.1) “an established practice of meeting with patients upon request to answer questions about financing the costs of their cancer care” as fundamental to reduce risk of financial distress, setting an expectation that it should be implemented by organizations of any size/resource level. Panelists recognized the enhanced guideline (2.3.4) “processes for integrating financial advocacy into existing cancer care planning and services…and facilitating regular multidisciplinary cancer care team communication regarding patients’ financial concerns and resulting psychosocial/emotional or medical impacts….” as an ideal practice that may only be feasible for larger or well-resourced organizations or more established financial advocacy programs.
The Guidelines reflect the broad spectrum of services that financial advocacy programs provide to patients and their caregivers. The inability to agree on being minimum or enhanced services or functions for the other 41 guidelines is likely due to the diversity of practice settings that is represented among panelists, as well as variability in the field in how financial advocacy services are currently delivered (or not)—bolstering the call for standardization.
Implications for Implementation by Psychosocial Providers
Panelists provided thoughtful comments on considerations for implementation that are fully detailed in the open-access report on ACCC’s website.24 Panelists agreed that “successful implementation will require a supportive environment, including recognition from leadership, decision makers, and provider champions that financial advocacy services are a key component of comprehensive, high-quality cancer care.” They also noted that it will be difficult to scale these services without investment, such as budget for staffing, physical space, training, technology, and other resources.
For Domain 1 (Financial Advocacy Services & Functions), the timeliness of benefits verification and prior authorization is stressed to enable informed decision-making. Panelists noted that completing these tasks 24 hours prior to any appointment is ideal to avoid unnecessary OOP expenses and avoid loss of revenue for the healthcare organization. Panelists also emphasized the importance of insurance education, which should include a conversation and providing transparent and written information to patients. Financial distress screening is a critical service, and healthcare organizations are encouraged to find a feasible method to screen all patients with cancer at least once, which may help reduce bias in screening selectively and reduce stigma around discussing financial concerns related to healthcare. Khera et al26 similarly call for a universal screening strategy and discuss its challenges and solutions. A process for following up on screening is essential—provision of financial assistance is a core service, and there are a variety of ways to secure financial and material support for patients in need.
For Domain 2 (Program Management Functions), the task force recognizes that healthcare organizations vary greatly in their structure and available resources for delivering financial advocacy services. A key activity in establishing a new program and sustaining or expanding existing services is generating buy-in, awareness of and concern for financial distress among leadership and the entire multidisciplinary care team. Strategies include staff education and cultivating a diverse workforce that reflects communities served. When feasible, financial advocacy is ideally supported through electronic systems, and program staff should protect patient confidentiality and adhere to their preferences for disclosure of sensitive financial information.
Domain 3 (Partner Engagement Functions) focuses on how financial advocacy team members become aware of resources for providing financial assistance and other support, which is often done through individual relationship building, although some databases of resources exist (eg, United Way’s 211.org; FindHelp.org; Patient Advocate Foundation’s National Financial Resource Directory). Resources are also available to help program administrators and staff learn how to develop financial advocacy and patient navigation programs (eg, ACCC’s Financial Advocacy Network, the Academy of Oncology Nurse & Patient Navigators, and the American Cancer Society National Navigation Roundtable).
The Guidelines can be used by healthcare organizations that wish to develop new or improve existing financial advocacy programs. The Guidelines represent multidisciplinary expert consensus on important services and functions in financial advocacy. The belief of the task force is that healthcare organizations should implement as many of the financial advocacy services in the Guidelines as feasible. However, the task force also recognizes that rigorous research is needed to evaluate whether adherence to the Guidelines works to improve care for patients. For brand new programs, beginning with minimum guideline 1.1.1 would be a starting point. For programs looking to improve, ACCC developed an assessment tool for organizations to assess their baseline status in concordance with the Guidelines and develop a plan to improve alignment; this could help generate baseline evidence to advance the implementation research called for by Doherty et al.7
Next Steps
Comprehensive uptake of these Guidelines is likely not immediately feasible for all healthcare organizations that are not currently providing most or any of the services and functions outlined. Further research to identify the minimum services needed for financial advocacy programs would be helpful to guide healthcare organizations on their initial investments and programming, allowing them to maximize impact for patients and themselves. In addition to more research to validate the core components of oncology financial advocacy as an intervention, scholars could research how reimbursement codes for principal illness navigation and social determinants of health screening can be applied to financial advocacy services. Scholars may also consider how oncology financial advocacy fits more broadly across the cancer continuum, expanding on the current Guidelines that focus on diagnosis- and treatment-related services, to include screening- and survivorship-related services.
The authors recognize that in the absence of broader policy and systematic changes related to insurance access, healthcare affordability, and accountability metrics for financial distress, widespread adoption of these guidelines may be challenging or limited. Healthcare leaders could look for opportunities to leverage quantitative and narrative data from patients to educate policy makers about the need and positive impacts of financial advocacy in advancing health equity, to help move supportive policies forward.
Strengths and Limitations
A major strength of this study is its timeliness to fill an evidence gap by providing consensus-based guidance to advance standardization in the field. The Delphi technique has many strengths, including leveraging broad expertise. Limitations include the paucity of rigorous evidence on the core components of oncology financial advocacy and inability to achieve more narrowed consensus among panelists on guidelines being minimum or enhanced; however, based on the near-even split in many votes, the task force felt that further rounds of voting would not be fruitful at this time.
Conclusion
ACCC led a rigorous and engaged Delphi study to develop 43 Financial Advocacy Services Guidelines. These Guidelines offer an important opportunity for advancing equitable, high-quality, and comprehensive cancer care delivery by informing how organizations can educate, screen for, and proactively intervene to reduce patients’ risk of financial distress. The lack of agreement about some being minimum or enhanced guidelines reflects the diversity of current practice and organizational resourcing and supports the need for standardization in the field. To reduce the impacts of financial distress on patients with cancer, expert consensus suggests that healthcare organizations should adhere to as many of the Guidelines as possible. Implementation of the Guidelines can also complement and align with cancer centers’ health equity and patient navigation priorities. Given their role in distress screening and needs navigation, navigators play a critical role in the design and delivery of financial advocacy services.
Support
The activities of the ACCC’s Financial Advocacy Network, including the present research study, are supported by Bristol Myers Squibb, Pfizer, Daiichi-Sankyo, Genentech, Janssen, Pharmacyclics, and Sanofi.
Acknowledgments
The authors would like to thank ACCC’s Financial Advocacy Network partners, including the Academy of Oncology Nurse & Patient Navigators, Triage Cancer, CancerCare, and the National Patient Advocate Foundation, and the Delphi panel participants for their contributions to the development of the Guidelines. The authors also thank Dr Margaret Liang for her feedback.
References
- Gordon LG, Merollini KMD, Lowe A, Chan RJ. A systematic review of financial toxicity among cancer survivors: we can’t pay the co-pay. Patient. 2017;10:295-309.
- Tucker-Seeley RD, Abel GA, Uno H, Prigerson H. Financial hardship and the intensity of medical care received near death. Psychooncology. 2015;24:572-578.
- Ramsey SD, Bansal A, Fedorenko CR, et al. Financial insolvency as a risk factor for early mortality among patients with cancer. J Clin Oncol. 2016;34:980-986.
- Carrera PM, Kantarjian HM, Blinder VS. The financial burden and distress of patients with cancer: understanding and stepping-up action on the financial toxicity of cancer treatment. CA Cancer J Clin. 2018;68:153-165.
- Yabroff KR, Han X, Song W, et al. Association of medical financial hardship and mortality among cancer survivors in the United States. J Natl Cancer Inst. 2022;114:863-870.
- Lentz R, Benson AB, Kircher S. Financial toxicity in cancer care: prevalence, causes, consequences, and reduction strategies. J Surg Oncol. 2019;120:85-92.
- Doherty MJ, Thom B, Gany F. Evidence of the feasibility and preliminary efficacy of oncology financial navigation: a scoping review. Cancer Epidemiol Biomarkers Prev. 2021;30:1778-1784.
- Shankaran V, Leahy T, Steelquist J, et al. Pilot feasibility study of an oncology financial navigation program. J Oncol Pract. 2018;14:e122-e129.
- Banegas MP, Dickerson JF, Friedman NL, et al. Evaluation of a novel financial navigator pilot to address patient concerns about medical care costs. Perm J. 2019;23:18-084.
- Wheeler SB, Biddell CB, Manning ML, et al. Lessening the Impact of Financial Toxicity (LIFT): a protocol for a multi-site, single-arm trial examining the effect of financial navigation on financial toxicity in adult patients with cancer in rural and non-rural settings. Trials. 2022;23:839.
- Kircher SM, Yarber J, Rutsohn J, et al. Piloting a financial counseling intervention for patients with cancer receiving chemotherapy. J Oncol Pract. 2019;15:e202-e210.
- Watabayashi K, Steelquist J, Overstreet KA, et al. A pilot study of a comprehensive financial navigation program in patients with cancer and caregivers. J Natl Compr Canc Netw. 2020;18:1366-1373.
- Wheeler SB, Birken SA, Wagi CR, et al. Core functions of a financial navigation intervention: an in-depth assessment of the Lessening the Impact of Financial Toxicity (LIFT) intervention to inform adaptation and scale-up in diverse oncology care settings. Front Health Servrv. 2022;2:958831.
- Wheeler SB, Rodriguez-O’Donnell J, Rogers C, et al. Reducing cancer-related financial toxicity through financial navigation: results from a pilot intervention. Cancer Epidemiol Biomarkers Prev. 2020;29:694.
- Chelsea NN, Reyes MF, Hsieh TYJ, et al. Implementation of financial toxicity screening and a novel financial navigation program. JCO Oncol Pract. 2023;19(suppl). Abstract 290.
- Henrikson NB, Schneider JL, King DA, et al. “It was just right:” patient experience, acceptability, and perceived utility of a novel financial navigation program in oncology. JCO Oncol Pract. 2023;19(suppl). Abstract 279.
- Henrikson NB, Anderson ML, Dickerson J, et al. The Cancer Financial Experience (CAFÉ) study: randomized controlled trial of a financial navigation intervention to address cancer-related financial hardship. Trials. 2022;23:402.
- Kirchhoff AC, Mann K, Waters AR, et al. A pilot intervention to improve health insurance literacy and financial toxicity among recently diagnosed adolescents and young adults with cancer. J Clin Oncol. 2022;40(suppl). Abstract 218.
- Offodile AC, Gallagher K, Angove R, et al. Financial navigation in cancer care delivery: state of the evidence, opportunities for research, and future directions. J Clin Oncol. 2022;40:2291-2294.
- Association of Community Cancer Centers. Trends in Cancer Programs. 2016. www.accc-cancer.org/docs/Documents/Surveys/trends-in-cancer-programs-2016
- Bell-Brown A, Watabayashi K, Delaney D, et al. Assessment of financial screening and navigation capabilities at National Cancer Institute community oncology clinics. JNCI Cancer Spectr. 2023;7(5)pkad055.
- McLouth LE, Nightingale CL, Dressler EV, et al. Current practices for screening and addressing financial hardship within the NCI Community Oncology Research Program. Cancer Epidemiol Biomarkers Prev. 2021;30:669-675.
- Association of Community Cancer Centers. Financial Advocacy Services Guidelines. 2018. www.accc-cancer.org/docs/documents/publications/financialadvocacyservicesguidelines.pdf
- Association of Community Cancer Centers. Financial Advocacy Guidelines. 2023. www.accc-cancer.org/home/learn/financial-advocacy/guidelines
- Tucker-Seeley RD, Thorpe RJ. Material-psychosocial-behavioral aspects of financial hardship: a conceptual model for cancer prevention. Gerontologist. 2019;59(suppl 1):S88-S93.
- University of Southern California. Reginald Tucker-Seeley measures more than money. Accessed July 17, 2025. https://gero.usc.edu/2017/06/11/measuring-more-than-money-copy/
- FACIT.org. COST: A FACIT Measure of Financial Toxicity. Accessed December 8, 2022. www.facit.org/measures/FACIT-COST
- National Comprehensive Cancer Network. NCCN Distress Thermometer and Problem List. Accessed December 8, 2022. www.nccn.org/global/what-we-do/distress-thermometer-tool-translations
- Doherty M, Jacoby J, Copeland A, et al. Building organizational capacity to deliver oncology financial advocacy. J Oncol Navig Surviv. 2023;14:203-210.
- Khera N, Holland JC, Griffin JM. Setting the stage for universal financial distress screening in routine cancer care. Cancer. 2017;123:4092-4096.