Korinne G. Lee, MSN, FNP-C1; Amanda Pate, MSN, RN-BC, OCN, ONS1; Bob Gold2; Jeff Rusk1; Chevon Rariy, MD1
1Oncology Care Partners; 2GoMo Health
Providing oncology care outside the clinic walls, where most side effects take place, can be extremely challenging. Most patients lack the requisite knowledge regarding the management of adverse events related to their diagnosis and treatment, which often results in increased emergency department visits and hospital admissions, increased morbidity, and a decrease in quality of life.1
Historically, home care has consisted of remote, telephonic nurse triage. However, many patients continue to cite limited telephonic access to healthcare providers as a cause of low patient satisfaction.2 Delivering quality care at home between clinic visits as an extension of doctors’ care is powerful when using a strategic synergy of technology coupled with human care. This case presents an elderly oncology patient successfully navigating a virtual platform to complete a survey, which triggered a remote nurse triage assessment, and escalation to a provider for symptom management and referral assistance. Barriers to care in this case are advanced age and education and health literacy gaps, in addition to the patient’s hesitancy to discuss her symptoms while face-to-face at a clinic visit. The program aimed to align care coordination, symptom management, and patient engagement with the objective of avoiding hospital admissions, reducing costs, and improving patient satisfaction.
Case Presentation
A 91-year-old female patient with stage IV breast cancer metastatic to the bone, on hormonal therapy, and residing in an assisted living apartment was recently seen in clinic by her oncologist. Based on her clinical profile and risk characteristics, her oncologist completed a referral to the patient-centric oncology navigation program that was supporting the practice. After her appointment, a virtual survey was sent to her mobile phone. She responded to the survey after clinic operating hours with responses that warranted immediate escalation to the virtual nurse. Her responses revealed that she was suffering from low levels of nausea, poor appetite, and weakness. The virtual nurse called the patient to perform a telephonic assessment in real time and determined that the patient was very weak and anxious. The patient was unsure how to manage her symptoms and was afraid of falling. Although she did have a walker, she told the nurse that she had been staying in bed because she was uncomfortable from the nausea, adding to her weakness. She reported loss of appetite due to nausea and discomfort, which further exacerbated her weakness. She voiced concerns about not yet having received physical therapy as prescribed by her primary care provider. She verbalized feelings of uncertainty and worry.
Due to the complexity and nature of her needs, the virtual nurse navigator escalated this case to a provider for a remote telehealth video visit. The provider could see that the patient was lying in bed looking exhausted and uncomfortable, but she was not in distress, excruciating pain, struggling to breathe, or experiencing any other worrisome symptoms. After a thorough assessment and discussion regarding her symptoms, she was guided on properly taking her prescribed antinausea medication, which she had avoided because she was unclear about the instructions. The patient was advised exactly when and how to take her medication and what foods to eat to help with her symptoms; she was also given information on the purpose and goals of physical therapy. A discussion was had with the patient to better understand her concerns, treatment expectations, and her wishes around her goals of care. A referral for nutrition assistance was placed, and the virtual care team was tasked with arranging meal assistance during business hours the next day.
The patient was already more comfortable by the end of the visit and had a plan for what would take place afterwards. The case was discussed with the medical oncologist who then scheduled the patient for an early follow-up visit to discuss her symptoms and palliative care options. The primary care doctor was notified to ensure on-site physical therapy was arranged. The ability to intervene early was essential in providing the much-needed supportive care and education to manage her symptoms before they intensified to the point of requiring hospitalization. She had been overwhelmed by the complexity of her medications, managing her symptoms, and coordinating her care. The access to immediate assistance after clinic operating hours provided by the high-tech, high-touch oncology care program was the kind of access to care that this patient needed and benefited from. In addition to the immediate escalation made possible by a patient’s direct-to-mobile survey responses, the oncology clinical care navigators develop longitudinal patient relationships facilitating proactive outreach. The frequency or “dose” of intervention is tailored to a patient’s needs based on clinical, social, and side-effect risk characteristics. For this patient, side effects were addressed in addition to facilitating discussions to ensure that goal-concordant care was addressed, thereby saving a trip to the emergency department. Discussions also helped facilitate palliative care options.
Discussion
There are a few important points to note from this case study. In a situation involving advanced illness, the program offered care coordination, symptom management, and referral management and also facilitated goal-concordant care discussions between the patient and the providers. Through a coordination of technology and virtual care, the program includes modalities to address behavioral health and social issues and close gaps in care such as access to transportation, healthcare services, and social services.
The platform offers 24/7 access to a live clinical care team and a virtual coach providing personalized educational support, as shown in Figure 1. This virtual clinical navigation team is available anytime over SMS, phone call, or email. This same team receives the escalation notifications whenever patients respond to any of the bidirectional messages or survey responses in a way that warrants clinical attention. All members of the unique population engaged in this program were over the age of 65 years, a testament to its intuitive user interface. The program overall has boasted a high engagement rate of over 75%, highlighting successful patient contact and involvement in their care plans. Much of this success can be attributed to the patented BehavioralRx approach—a unique technological blend of behavioral and cognitive science carefully crafted to generate trust and enhance human resilience.
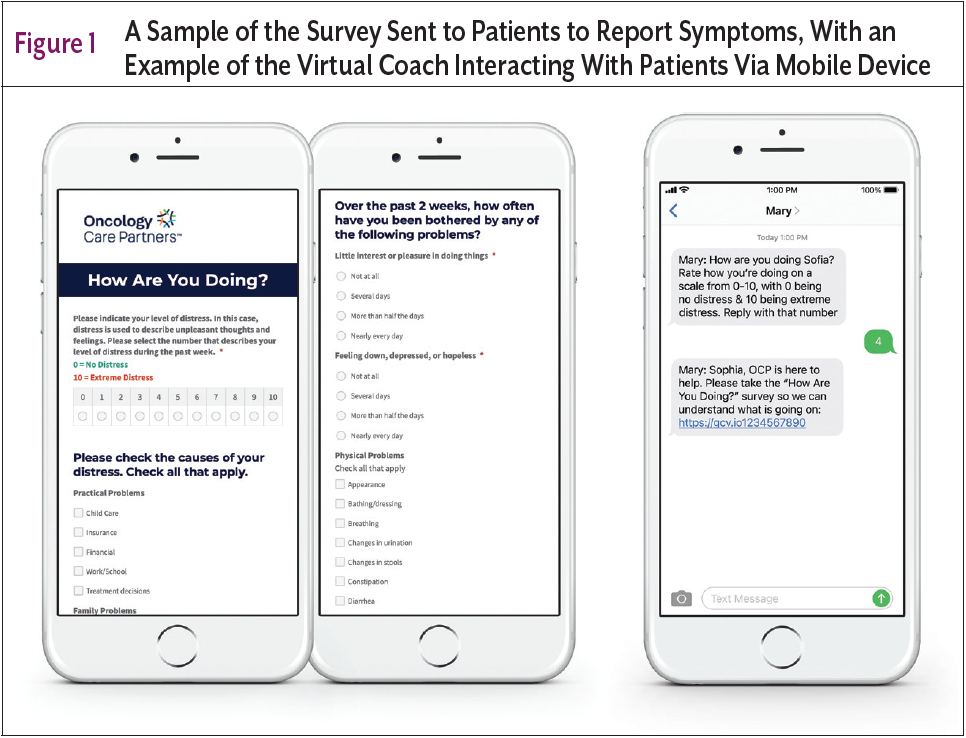
This case describes a 91-year-old patient who was easily able to use this technology by tapping on a texted link sent to her by the AI-enabled texting program. The provided link navigated her to a survey to assess her physical, mental, and social well-being. Studies have shown that patients more frequently reported symptoms on a self-assessment tool rather than on a clinical assessment performed by a provider, thus the ability and convenience to conduct an assessment from home was particularly important.3 Ensuring that the survey is user friendly with radio buttons to select in each category ensures accurate responses and decreases confusion and ambiguity. The platform uses an AI-driven virtual coach that provides tailored educational support and resources. The messaging platform has functionality that can send bidirectional messages to elicit a direct response from the patient. Those questions prompt the patient to respond and, based on response, escalate their needs or problems to a remote human provider. Additionally, patients can initiate contact with the AI platform first by using texted-in keywords to gain real-time access to information that may be useful to them in the moment. For this particular program, participants are able to text in “CARE” at any time to be directed to the survey discussed previously.
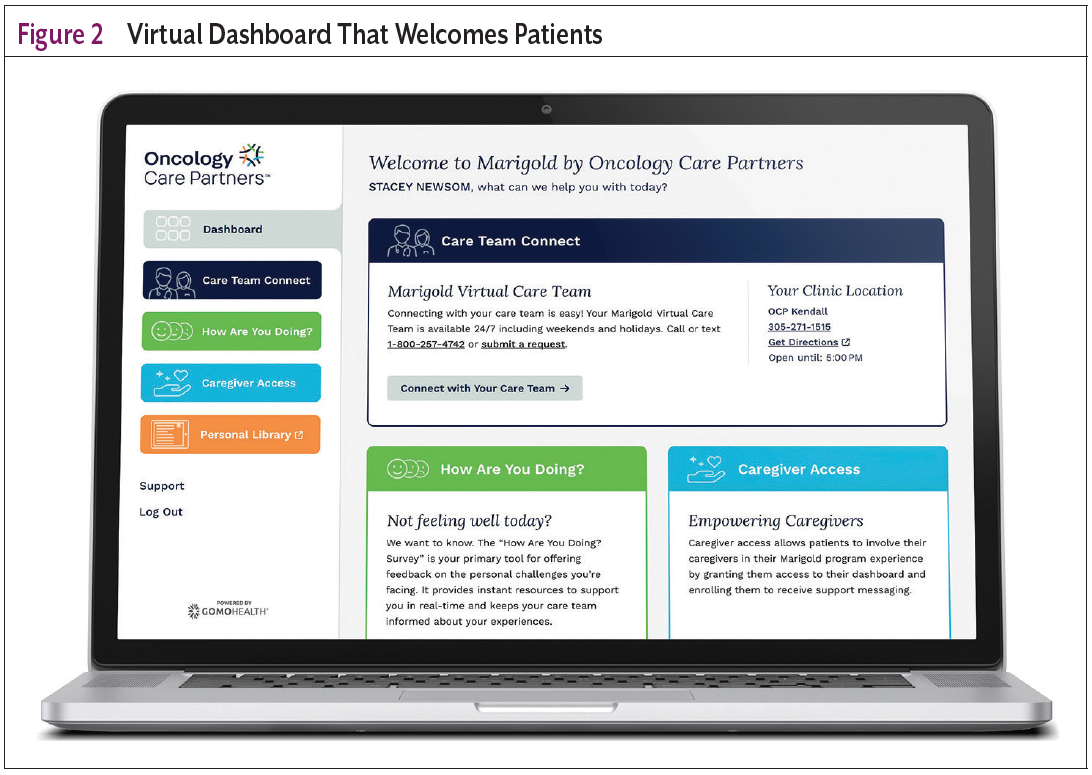
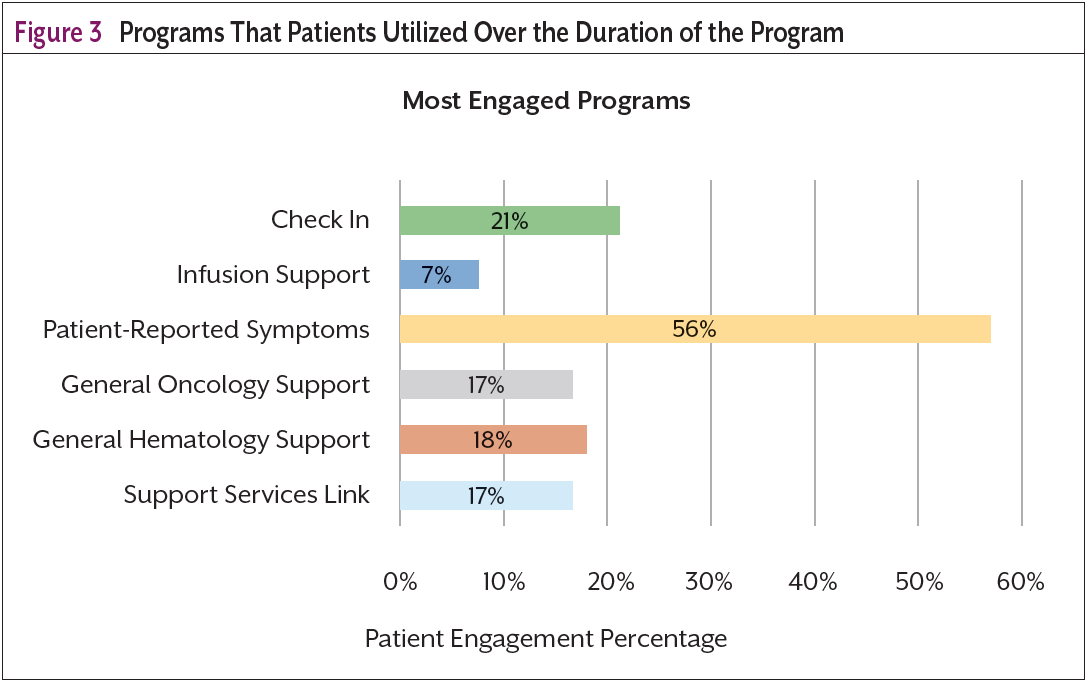
In addition to the seamless messaging programs, a patient dashboard, as seen in Figure 2, offers additional support and supplemental educational material for the patient and their caregivers. Through this dashboard, patients can access their medical records as well as a library of educational materials tailored to their physical, social, and emotional needs (resources that have often also been sent to them via links in the SMS messaging program). The patient dashboard provides an example of how integrating multiple patient data sets can create a more holistic view of the patient, (Figure 3), both for the patient and the care team. The dashboard relies on direct electronic medical record (EMR) data access—combining live medical record access with live patient outcomes from both self-assessments and virtual provider assessments. It is important to note that this is made possible by an EMR application that provides robust application programming interface (API) libraries to send and receive data. Additionally, algorithms are applied to the EMR data to make data more human-readable and patient friendly (eg, consolidating and simplifying a patient’s multiple diagnosis codes into the key cancer diagnosis “breast cancer”). Through the portal, patients are also able to enroll a caregiver to receive supportive care messaging to ease the caregiver burden and stress associated with caring for a loved one with cancer.
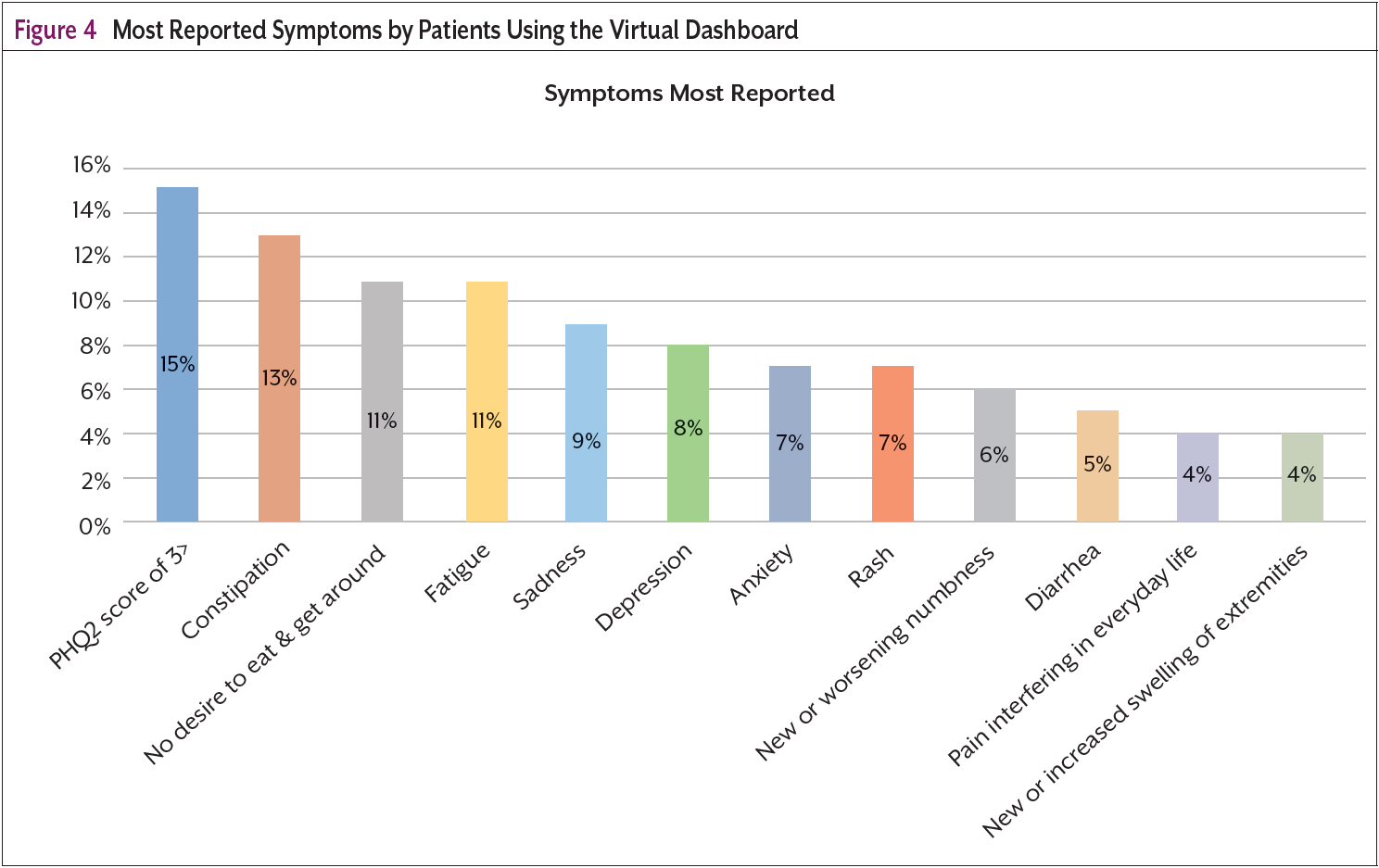
The most common self-reported symptoms on the survey as shown in Figure 4, are depression or sadness, constipation, fatigue, and lack of the desire to eat. Many of these were not reported in clinical visits with the on-site provider. These symptoms are crucial for early identification and intervention to aid in providing care when needed and in keeping patients out of the hospital. Intervention and resolution of these symptoms also keeps patients healthy enough to continue keeping their oncology appointments and adhering to treatment plans. Timely access to care at home made possible by coupling high-touch technology with a human-centric approach is not only effective but is also changing the landscape of cancer care navigation. The use of AI has allowed us the ability to combine machine intelligence with the critical thinking and compassion of human experts resulting in concise and timely interventions and an improved patient experience.4
The case demonstrates how a sophisticated oncology navigation program can directly contribute to cost-savings and a positive return on investment. By ensuring timely and proactive symptom relief and subsequent follow-ups and coordinated care, such programs can lower the rate of emergency department visits and hospital readmissions. The program helped to streamline care pathways, ensuring the patient received the right type of care at the right time, minimizing unnecessary tests, treatments, or hospital stays. Navigators support patients in adhering to their treatment plans, leading to better outcomes and reducing the need for costly interventions due to complications. Navigators can help to facilitate goal-concordant care discussions with both patients and providers, including palliative care and end-of-life conversations. The results are a better patient experience through increased engagement and retention and enhanced provider satisfaction due to the availability of deeper insights into patients’ lives. This allows the care team to better coordinate with multiple healthcare constituents and ultimately improves the overall care the patient receives. This innovative approach drives the expanded Quadruple Aim forward by enhancing patient experience, improving population health, lowering healthcare costs, and empowering care teams to deliver personalized, efficient care.5 Timely wraparound care, powered by AI and human expertise, is revolutionizing cancer care by enabling early symptom intervention, improving outcomes, and ensuring patients stay on track with their treatment plans.
Acknowledgments
The authors would like to thank Oncology Care Partners for their trusted care and support with this program and GoMo Health for providing the patient engagement platform technology.
References
- Krzyzanowska MK, Treacy J, Maloney B, et al. Development of a patient registry to evaluate hospital admissions related to chemotherapy toxicity in a community cancer center. J Oncol Pract. 2005;1:15-19.
- Richard ML, Parmar MP, Calestagne PP, McVey L. Seeking patient feedback: an important dimension of quality in cancer care. J Nurs Care Qual. 2010;25:344-351.
- Basch E. The missing voice of patients in drug-safety reporting. N Engl J Med. 2010;362:865-869.
- Biancalana M. Artificial intelligence in oncology: the winds, the challenges, and how we can deliver on personalized cancer care. J Clin Pathways. 2023;9:55-59.
- Bodenheimer T, Sinsky C. From triple to quadruple aim: care of the patient requires care of the provider. Ann Fam Med. 2024;12:573-576.